Keywords
Phototherapy, Narrowband UV-B, UV therapy, Psoriasis, Excimer laser
Key points
- •
Phototherapy with UV light can be used in the treatment of several cutaneous disorders.
- •
Phototherapy is an efficacious treatment option in the management of psoriasis and should be a first therapy considered in patients with moderate-to-severe plaque psoriasis.
- •
Narrowband UV-B is used as the first-line phototherapy treatment option for moderate-to-severe psoriasis due to its clinical efficacy and mild side-effect profile.
- •
Targeted UV-B therapy phototherapy and employment of excimer lasers are excellent options for patients with more limited disease, although there are now reports of use for extensive disease.
Introduction
Definition
Phototherapy refers to the use of nonionizing radiation, from the UV range, in the treatment of skin disorders ( Table 2.1 ). It represents an efficacious, cost-effective, and generally nonimmunosuppressive staple in the management of psoriasis.
| UV Spectrum (10–400 nm) | |
|---|---|
| Abbreviation | Wavelength (nm) |
| UV-A | 320–400 |
| UV-B | 290–320 |
| UV-C | 200–290 |
History
The use of sunlight in the treatment of cutaneous diseases can be traced back to ancient times. Evidence dating thousands of years demonstrates the use of plant extracts, including those from the Ammi majus plant (psoralens), followed by sun exposure to treat vitiligo in Egypt and India. However, it was not until the late nineteenth century that heralded major advances in the development and use of phototherapy. In 1901, Niels Ryberg Finsen published the results of the treatment of lupus vulgaris with a carbon arc lamp, which marked a breakthrough in the treatment of skin diseases. For this, Finsen received a Nobel Prize in medicine, the first and only one ever awarded in the field of dermatology.
Shortly after in 1925, William Goeckerman combined the use of UV radiation with coal tar in the treatment of psoriasis. The Goeckerman regimen as it came to be known would remain a mainstay in phototherapy treatment of psoriasis for several decades. A major shortcoming of the Goeckerman regimen was the low output of the lamps. However, in 1978, Wiskemann introduced broadband UV-B radiation in a closed chamber to treat psoriasis, which mitigated this drawback. Despite these advances, broadband UV-B radiation was less efficacious than psoralens followed by UV-A radiation, also known as PUVA therapy, and as a result, did not gain widespread popularity. It was not until the late 1970s when Parrish and Jaenicke determined the action spectrum of psoriasis with a peak response at 313 nm that gave impetus to narrowband (NB) UV-B as a new phototherapeutic modality. In 1988, both Van Weelden and colleagues and Green and colleagues demonstrated the superior clinical efficacy of NB UV-B and subsequently marked the decline of broadband-UV-B (BB-UV-B) use for psoriasis.
Types
This chapter provides an overview of UVB phototherapy in the management of psoriasis.
Broadband ultraviolet B (290–320 nm)
Broadband (BB) UV-B phototherapy was initially described in the Goeckerman regimen in 1925. For many decades, BB-UV-B remained an option in the psoriasis treatment arsenal despite being less efficacious than other treatment modalities. Presently, however, BB-UV-B has largely been replaced by NB-UV-B radiation, which has demonstrated superior efficacy in clearing psoriatic lesions.
Narrowband ultraviolet B (311–313 nm)
First defined in 1976, NB-UV-B has taken the place of BB-UV-B in the treatment and management of psoriasis. NB-UV-B has gained popularity over PUVA in the treatment of psoriasis for several reasons. First, NB-UV-B had similar efficacy rates compared with PUVA. Therefore, NB-UV-B is generally favored over PUVA due to greater ease of use for the patient. Another factor is the increased risk of squamous cell cancer (SCC) associated with PUVA treatments. The risk of SCC increases as the number of PUVA treatments increases. NB-UV-B phototherapy has not been shown to incur any increased risk of skin cancer. Last, NB-UV-B is safe to use in children and pregnant patients and lacks psoralen-related side effects, which ultimately makes it more favorable as an initial phototherapy modality.
Targeted phototherapy
Targeted phototherapy is a method of phototherapy in which only affected areas of skin are treated. Various devices can be used to deliver focused UV-B radiation on skin lesions while sparing uninvolved skin. These devices include high fluence devices, like the excimer laser and flash lamp, and lower output devices, like UV-B light-emitting diodes. Introduced in 1997, the 308-nm excimer laser contains an unstable mixture of xenon and chloride, which form “excited dimmers.” It is the dissociation of these dimers that produces the monochromatic wavelength, which is transmitted via a fiber-optic cable to the lesion. The excimer laser allows for targeted therapy that spares uninvolved skin, especially in areas that are otherwise difficult to treat, like the scalp, hands, and feet. In addition, it can generate high fluencies of UV-B, resulting in faster clearing and fewer exposures. Although the excimer laser is not suitable for large body surface areas because the treatment may be considerably resource intensive and lengthy, the availability of more powerful UV emitting devices (and aggressive treatment protocol) is extending the range of area that can be treated. Although targeted treatment has generally been used for mild, localized psoriasis, it can also be used for severe psoriasis of the palms/soles or even for extensive disease.
Tanning beds
The use of commercial tanning beds may be a viable alternative for patients in which in-office and home phototherapy are either unaccessible or impractical. Although evidence to support the routine use of tanning beds may be sparse, approximately 36% to 52% of patients have used tanning beds in the treatment of their psoriasis. However, given the increased risk of skin cancer and full-body UV exposure, tanning bed use remains controversial, and not all dermatologists agree that they should be used.
Indications
Indications for UV-B radiation include psoriasis, atopic dermatitis, vitiligo, and mycosis fungoides, among several others ( Table 2.2 ).
| Common | Less Common |
|---|---|
| Psoriasis Vitiligo Atopic dermatitis Mycosis fungoides Pruritus (associated with renal disease, polycythemia vera) | Acquired perforating dermatosis Chronic urticaria Cutaneous graft-versus-host disease Polymorphous light eruption Cutaneous mastocytosis Granuloma annulare Lichen planus Lichen simplex chronicus Lymphomatoid papulosis Parapsoriasis Pityriasis lichenoides Pityriasis rosea Pityriasis rubra pilaris Seborrheic dermatitis |
Mechanism of action
The epidermal layer of human skin, composed primarily of keratinocytes, absorbs most UV radiation, with only the longer wavelengths having the ability to penetrate the dermis. It was thought that UV-B’s antiproliferative properties were a result of direct DNA damage; however, recent evidence suggests that phototherapy also exerts immunomodulatory effects. Specifically, UV-B radiation diminishes type-1 T-cell predominance by altering cytokine profiles, induces apoptosis of keratinocytes and T cells, and depletes Langerhan cell numbers.
Human T helper (Th) lymphocytes can be separated into T effector cells, which protect the body from pathogens, and regulatory T cells, which dampen immune responses when they become dangerous to the host. Different subsets of effector T helper cells are distinguished based on their cytokine production profiles in addition to transcription factors and homing receptor expression. The main T helper subsets include Th1, Th2, and Th17. In psoriasis, it is the Th1/Th17 T cells that overexpress Th1 and Th17 cytokines, which, in turn, influence the hyperproliferation of keratinocytes and the resultant inflammation.
UV-B radiation shifts the dysregulated predominance of Th1/Th17-mediated immune response in psoriasis to more of a Th2 response. Specifically, UV-B phototherapy induces interleukin-10 (IL-10) production in human keratinocytes, which is a major regulatory cytokine in the Th2 pathway. In addition, phototherapy downregulates Th1/Th17 proinflammatory pathways by decreasing pathogenic cytokine (IL-23, IL-20, interferon-γ, IL-17, IL-22) production.
Furthermore, UV-B exerts its therapeutic effects by inducing apoptosis. Apoptosis is a process of programmed cell death in response to noxious stimuli. Evidence indicates that one mechanism in which UV-B clears psoriatic lesions is through the induction of apoptosis in keratinocytes, epidermal T cells, and to a lesser extent, Langerhans cells.
Last, UV-B is involved in promoting localized immunosuppression. In addition to apoptosis, UV-B radiation influences the migration of Langerhans cells from the epidermis as well as decreases dendritic cell expression of B7 costimulatory signals, which is necessary for the stimulation and activation of T cells.
Efficacy
Efficacy can be evaluated with regards to fluency, clearance, remission times, and number of treatments. The Psoriasis Area and Severity Index (PASI) score was developed as a tool to measure the severity of psoriasis. A variant of that score, the PASI-75, determines the percentage of patients that achieved 75% reduction in the baseline PASI score and is a common measure of treatment efficacy.
Broadband Ultraviolet B
UV-B radiation is efficacious in the treatment and management of psoriasis. By virtue of being discovered first, BB-UV-B has a longer safety record than NB-UV-B but is less efficacious in the treatment of psoriasis. Only selective BB-UV-B (305–325 nm) has shown evidence of being as effective as NB-UV-B in clearing chronic plaque psoriasis.
Narrowband Ultraviolet B
NB-UV-B phototherapy is an effective therapeutic option in the treatment of plaque psoriasis. In a systematic review of 41 randomized control trials, 68% of patients receiving NB-UV-B monotherapy achieved plaque clearance, whereas 62% achieved PASI-75. When compared with oral PUVA, NB-UV-B may be less efficacious in clearing lesions but favored overall because of less risk of adverse events and increased ease of use.
If NB-UV-B phototherapy alone is insufficient to manage a patient’s disease, then a combination of NB-UV-B plus topical or systemic adjuncts may be considered. Emollients, including petroleum jelly, mineral oil, and coal tar, may result in improved plaque clearance. In addition, calcipotriol and maxacalcitol (vitamin D analogues) and psoralens at higher concentrations may also facilitate lesion resolution. Regarding systemic adjuncts to NB-UV-B phototherapy, the addition of methotrexate to NB-UV-B renders the treatment more efficacious than NB-UV-B alone. Combining phototherapy with retinoids or cyclosporine decreases the cumulative NB-UV-B dose needed to clear psoriasis. Combination therapy using biologics may potentiate their efficacy, but sufficient data are lacking.
Data in children and pregnant women have also been promising, because 51% of pediatric patients achieved complete clearance and an additional 41% had a 75% reduction in their PASI score.
Targeted phototherapy
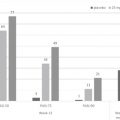
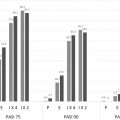
Recent meta-analyses using a PASI clearance of 75% evaluated the efficacy of targeted NB-UV-B in the treatment of plaque psoriasis and demonstrated efficacy rates for the excimer (308-nm) laser to be 70%, 59% for excimer (308-nm) light, and 49% for localized NB-UV-B (311–313-nm) light.
In addition, the excimer laser can clear psoriasis, with about 70% of patients having a 75% or greater reduction in their psoriatic lesions. Although partial clearance is possible in as few as one session, usually higher frequency treatments (2 to 3 per week) are considered to be more effective, with higher rates of complete clearance. In one multicenter trial for mild-to-moderate plaque-type psoriasis, 84% and 35% of subjects demonstrated PASI score improvement of at least 75% and 90%, respectively, after 10 or fewer treatments. In addition, the 308-nm excimer laser required fewer visits while remaining relatively effective when compared with whole-body phototherapy.
Similarly to NB-UV-B, combination therapies that use the excimer laser with topical adjuncts resulted in higher efficacy rates compared with monotherapy alone.
Tanning beds
Efficacy of commercial tanning is difficult to assess due to the lack of standardization of tanning bed devices and lamps as well as by the poor compliance of tanning regimens.
Although tanning beds primarily emit UVA radiation, approximately 0.5% to 5.0% of the total light output is within the UV-B spectrum. One controlled trial compared low UV-B output (0.7%) lamps to higher UV-B output (4.6%) lamps in the treatment of psoriasis and determined that when equal erythema doses were given, there was a similar significant improvement in PASI scores. In addition, higher output lamps achieved mean reductions in PASI scores of 35.4% ± 24.1% in 80% of patients.
Safety
UV-B is generally well tolerated and safe in almost all patients, including children and pregnant women. The most common acute side effect is “sunburn,” which is a red phototoxic reaction that occurs about 24 hours after treatment. Erythema is usually dose-dependent and has comparable rates between NB-UV-B versus BB-UV-B therapy. Pruritus has occasionally been described in psoriatic lesions following UV-B therapy. However, this may be due more to the underlying disease process rather than secondary to phototherapy. Hyperpigmentation is another common side effect of UV-B phototherapy that can interfere with treatment compliance depending on the patient’s tolerance of skin color changes. Pregnant patients should be informed of the possible increased risk of melasma secondary to UV-B phototherapy.
Other less common acute effects include blistering, cataract formation, and reactivation of herpes simplex virus infection. Blistering and painful erythema have been seen in approximately 16% of patients and may be caused by a quick reduction in acanthosis and desquamation before defensive mechanism, that is, pigmentation and increases in stratum corneum, take place. There have been a few cases reporting the reactivation of herpes simplex virus infection following phototherapy; therefore, precautionary measures should be taken in those prone to frequent relapses. UV-B phototherapy has not been associated with an increased risk of fetal abnormalities or prematurity and seems to be the safest therapy in extensive disease. However, overheating should be avoided due to the increased risk of neural tube defects.
The most common long-term effect is photoaging, which may present as wrinkling, lentigines, and telangiectasias. The most concerning long-term outcome is photocarcinogenesis. NB-UV-B probably confers less of a cancer risk compared with PUVA but may be 2 to 3 times more carcinogenic than BB-UV-B at similar doses. However, the risk of skin cancer in psoriasis patients treated with NB-UV-B correlated with the number of treatments, yet the overall risk of malignancy in the NB-UV-B-treated patients was not greater than in the general population. In addition, although NB-UV-B treatment has not been linked to any skin cancers, long-term follow-up data are lacking. Therefore, providers should continue counseling patients regarding skin cancer risk with NB-UV-B treatment. In addition, ongoing skin cancer monitoring of patients, in addition to genital and facial shielding, is recommended.
Targeted phototherapy
Evidence suggests that targeted phototherapy is safer than whole-body phototherapy by reducing the amount of unnecessary radiation. Adverse events are associated with higher cumulative UV-B doses and increased number of treatments.
Given its targeted nature, the adverse effects of the excimer laser are limited to the area that was targeted and are similar to those of NB-UV-B. Short-term effects include erythema, blistering, and hyperpigmentation. Blisters are noted more often with the use of higher doses. Hyperpigmentation may be psychologically distressful for patient; however, it tends to resolve with the discontinuation of treatment. Long-term safety data in patients treated with the excimer laser, including children and pregnant women, are lacking but generally considered to be safe.
Tanning beds
Unsupervised use of commercial tanning beds is problematic and increases the likelihood of acute side effects that include phototoxic reactions, blisters, and itching. Long term, there is an increased risk of developing melanoma, SCC, and basal cell carcinoma in patients who have ever used a recreational tanning bed compared with those who have not. In addition to history of use, younger age at first use and increased frequency of sessions incur greater risk of skin cancers in recreational tanners.
Precautions
Although normally safe in most patients, UV-B phototherapy is absolutely contraindicated in patients with xeroderma pigmentosum or lupus erythematosus ( Table 2.3 ).
| Absolute | Relative |
|---|---|
| Xeroderma pigmentosum Lupus erythematosus | Photosensitivity disorder Taking photosensitizing medications History of melanoma History of atypical nevi Multiple risk factors for melanoma History of multiple nonmelanoma skin cancers Immunosuppressed secondarily to organ transplant |
Related posts:



Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


