Keywords
Psoralen-UV-A, PUVA, Photochemotherapy, Psoriasis
Key points
- •
Psoralen-UV-A (PUVA) photochemotherapy involves use of either an oral or topical psoralen followed by exposure to long-wave UV-A radiation. This combination leads to a clinically beneficial phototoxic response, which has been used therapeutically for a wide array of dermatoses.
- •
PUVA is an effective form of therapy for chronic plaque-type psoriasis with the potential for induction of long-term remission.
- •
Use of PUVA photochemotherapy has become limited secondary to cumbersome administration, acute toxicity, the availability of alternative modalities, and, most notably, the risk of carcinogenesis.
- •
Although caution must be exercised when administering PUVA, it remains a viable treatment option for individuals with recalcitrant disease, darker skin types, and localized, refractory forms of psoriasis, such as palmoplantar pustulosis.
Introduction
Photochemotherapy broadly refers to a treatment method that uses a photosensitizing compound and ultraviolet radiation. Psoralen-UV-A (PUVA) therapy more specifically involves use of either an oral or a topical psoralen followed by exposure to long-wave UV-A radiation (320–400 nm). This combination leads to a clinically beneficial phototoxic response, which has been used therapeutically for a wide array of dermatoses. The use of psoralen photochemotherapy dates back thousands of years to ancient Egypt and India, where the pigment-inducing qualities of naturally occurring plants were anecdotally described and applied to pigmentary disorders such as vitiligo. The period ranging from the 1930s to 1960s saw the chemical and structural identification of psoralens with extraction and synthesis. PUVA, in its modern form, was established by 1947 for the treatment of vitiligo and was subsequently adapted for use in psoriasis by Pinkus in 1951. The development of a high-intensity UV-A light source in 1974 firmly established the use of this modality as a highly effective treatment of psoriasis. Over time, treatment options for psoriasis have expanded and regular use of PUVA therapy has declined because of its photocarcinogenic potential. This chapter discusses the mechanism of PUVA as well as efficacy, dosing, safety, and precautions.
Mechanism of action
Psoralens are furocoumarins that are either naturally derived or synthetically produced. Currently, in North America, 8-methoxypsoralen (8-MOP) is the only available oral and topical formulation, whereas in Europe, 5-methoxypsoralen (5-MOP) is used due to its lower potential for phototoxicity and reduced gastrointestinal side effects. Trimethylpsoralen (TMP) has been traditionally used for bath PUVA, a practice that has been chiefly used in Scandinavian countries. The lower phototoxic potential of TMP has also led to its use, primarily in South Asia, in combination with sunlight exposure.
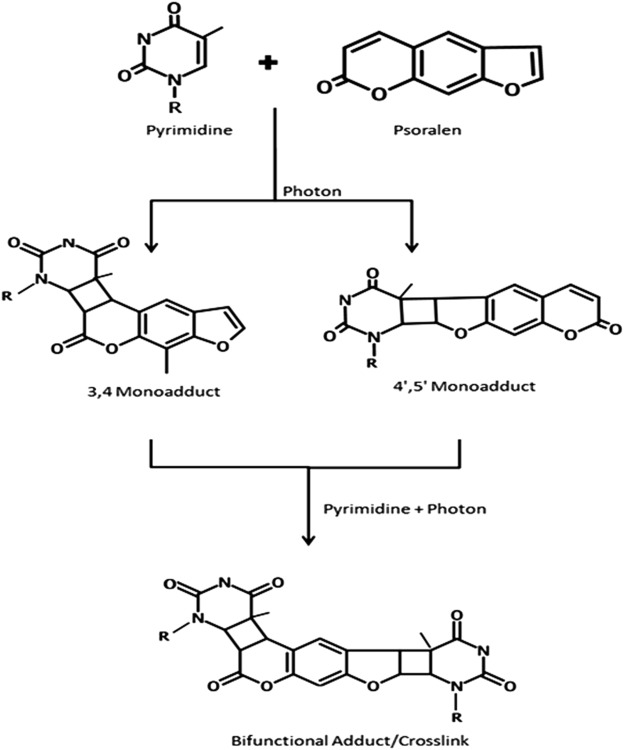
Following oral ingestion or topical application, the psoralen intercalates between DNA base pairs but remains quiescent in the absence of ultraviolet radiation. Upon initial exposure to UV-A, cyclobutane monoadducts are formed with pyrimidine bases. When a second photon of energy is absorbed, psoralen-DNA cross-linking occurs, which inhibits DNA replication and causes cell cycle arrest ( Fig. 3.1 ).
In addition to direct effects on cellular DNA, numerous changes in the cutaneous microenvironment have been observed following PUVA treatment. Psoralen photosensitization leads to altered cytokine secretion, including an increase in the expression of interleukins-1, -6, and -10 as well as immunosuppressive prostaglandins. Adhesion molecules and growth factor receptors are similarly modulated as is demonstrated by intercellular adhesion molecule-1, whose upregulation—a hallmark of inflammatory skin conditions—is effectively mitigated by photochemotherapy. Alteration in these mediators leads to transformation from a T helper 1 (Th1) and Th17 profile to a Th2 phenotype. Activated psoralens also interact with molecular oxygen, leading to the formation of reactive oxygen species. These reactive molecules and free radicals result in cell membrane damage by lipid peroxidation, disruption of mitochondria, and activation of eicosanoid pathways.
Following successful PUVA therapy, there is a decline in proliferating epidermal cells and a significant reduction in the epidermal thickness of psoriatic lesions. Current evidence suggests that this is mediated, in part, by induction of p53 and Fas pathways with subsequent keratinocyte apoptosis. There is evidence that differential expression of microRNAs plays a large role in p53-dependant apoptosis with significant upregulation of miR-4516 and increased Retinoic Acid Inducible Gene-1 signaling, leading to induction of autophagy and reduced cell migration.
Although effective at reducing epidermal keratinocyte proliferation, PUVA is far more potent at inducing apoptosis in lymphocytes, which may be related to suppression of Bcl-2 expression. In one in vitro study, there was virtual elimination of CD3 expression following bathwater treatment with either TMP or 8-MOP. The degree of lymphocyte depletion has been reported to correlate with clinical response.
A major advantage of PUVA over UV-B phototherapy is that UV-A penetrates deeper into the skin. As a result, cellular effects can be detected throughout the epidermis, papillary dermis, and superficial vascular plexus, leading to alterations in dermal dendritic cells, mast cells, endothelial cells, and infiltrating immune cell function.
Efficacy
Numerous studies have demonstrated the efficacy of PUVA in treating psoriasis. These studies include 2 early and integral investigations—one in the United States in 1977 and one in Europe in 1981—that firmly established PUVA as an effective therapeutic option. The American study used oral 8-MOP and high-intensity UV-A radiation. Of the 1139 patients included in the final analysis, clearance was noted in 88% and was reached at a mean of 23.6 treatments. Of note, clearance was defined as having macular erythema, hyperpigmentation, or normal-appearing skin. Initial dosing was based on skin phototype, and a fixed dose was used for escalation of therapy in the absence of erythema. In the European study, data from 18 separate institutions were pooled and evaluated. In agreement with the US cohort, 88.8% of the 3175 patients treated with PUVA achieved a response better than “marked improvement” over an average of 20 exposures. Dosing in this study was determined by the minimal phototoxicity dose, and subsequent adjustment was individualized to each patient. These findings were of paramount importance when considering that patients with severe, generalized involvement previously required inpatient hospitalization to achieve comparable results. Similarly, impressive response rates were noted in 2 comparative studies that evaluated the efficacy of PUVA in relation to narrowband (NB) UV-B. The PUVA-associated clearance rates reported in these studies were 70% and 84%, which, in both instances, were superior to NB-UV-B therapy. Clearance in these trials was defined as either 95% to 100% improvement or total clearance of psoriatic plaques above the knees, respectively. Of note, long-term remission (>6 months) was also achieved by a larger proportion of the subjects treated with PUVA (35% vs 12% in the NB-UV-B cohort).
A Cochrane Review formally comparing PUVA and NB-UV-B for the treatment of psoriasis was reported in 2013. As with most phototherapeutic interventions, the analyzed studies were confounded by disparate dosing strategies, frequency of use, and outcome measures. Of the 3 studies included, one revealed that NB-UV-B was as effective as oral PUVA, whereas the other 2 found PUVA to be superior to NB-UV-B. A European review similarly concluded that PUVA had superior efficacy, when compared with NB-UV-B, as well as a higher probability of remission at 6 months (odds ratio = 2.73; 95% confidence interval [CI] 1.19–6.27). The duration of remission has been correlated with Psoriasis Area and Severity Index scores at the end of treatment. In clinical practice, this difference in response and remission period must be weighed against the potential for carcinogenesis (to be discussed later in detail). Several studies have demonstrated that bath PUVA is not only as effective as orally administered PUVA but also requires a lower cumulative dose of UV-A and has fewer associated adverse effects. This treatment option, however, requires preparation of psoralen-containing bath water, immersion of the patient in the bathtub, and irradiation with UV-A immediately after completion of bathing. In light of the resources needed to properly administer bath PUVA, its use has been limited worldwide.
Combination Therapy
Effective combination regimens have been sought in an effort to reduce the cumulative dose of UV-A and potentially mitigate the associated risks. Topical corticosteroids, calcipotriol, and tazarotene are all considered synergistic with PUVA and carry minimal additional side effects. Concomitant exposure to NB-UV-B has also been investigated for use in recalcitrant cases. In a bilateral comparison study, patients were noted to reach clearance in an average of only 11.3 treatments with a mean cumulative UV-A dose that was less than half of what was given with PUVA monotherapy. Despite these findings, UV-B-PUVA combination therapy is not used due to concerns for increased photocarcinogenicity.
The combination of PUVA and oral retinoids has been well studied. In a randomized, placebo-controlled trial, 96% of subjects who received adjunctive acitretin therapy attained marked or complete clearance in comparison to 80% of subjects who received PUVA phototherapy alone. Significantly, the cumulative UV-A dose for patients in the acitretin/PUVA arm was 42% less than those who did not receive combination therapy. These findings are supported by another placebo-controlled trial, which found the combination of oral retinoids and PUVA to be superior in many regards, including a decrease in lesional scores, number of sessions, and total cumulative dose of UV-A required before clearance. On average, the patients in this study experience a decrease in treatment duration of 18 days when treated with concurrent PUVA and acitretin. The combination of these 2 therapies may also help to reduce the potential side effects. Not only is a lower cumulative dose of UV-A required but acitretin may also provide protection with regard to cutaneous malignancy. Because of the potential for increased carcinogenesis, concurrent treatment with cyclosporine is generally not recommended. The safety of combination therapy with methotrexate has also been challenged, although to a lesser degree.
Dosing
8-MOP is available orally in a variety of preparations, including crystals, micronized crystals, and a liquid, which has a higher, earlier, and more reproducible peak concentration. The liquid formulation enclosed in a soft gel capsule is currently the most widely available. Following ingestion, oral psoralens are metabolized in the liver and ultimately renally excreted after 12 to 24 hours. Psoralens are subject to a first-pass effect that can lead to drastic variability in plasma concentration following slight alterations in administration. The initial dose of psoralen is based on the patient’s weight, as outlined in Table 3.1 . UV-A should be delivered 1 hour following ingestion, with the initial UV-A dose dependent on the patient’s phototype. Table 3.2 lists dosing guidelines. Ideally, patients should refrain from eating 1 hour before and 1 hour after dosing because food impairs the absorption of methoxypsoralen. Strict adherence to fasting is not usually feasible, however, as ingestion of psoralens on an empty stomach can lead to gastrointestinal side effects such as nausea, and less commonly, vomiting. In practice, most practitioners recommend that the psoralen be taken with a small meal. Care must be taken to ensure that the type of food, amount of food, and the time interval between the meal and psoralen dosing are held constant to minimize variations in the serum levels. For topical PUVA therapy, 0.1% 8-MOP in an emollient base is recommended and should be applied 30 minutes before exposure to UV-A starting at a dose of 0.25 to 0.5 J/cm 2 and increasing by 0.25 to 0.5 J/cm 2 as tolerated.
| Patient’s Weight | ||
|---|---|---|
| lb | kg | Dose (mg) |
| <66 | <30 | 10 |
| 66–143 | 30–65 | 20 |
| 144–200 | 66–91 | 30 |
| >200 | >91 | 40 |
| Skin Type | Initial Dose (J/cm 2 ) | Increments (J/cm 2 ) | Maximum Dose (J/cm 2 ) |
|---|---|---|---|
| I | 0.5 | 0.5 | 8 |
| II | 1.0 | 0.5 | 8 |
| III | 1.5 | 1.0 | 12 |
| IV | 2.0 | 1.0 | 12 |
| V | 2.5 | 1.5 | 20 |
| VI | 3.0 | 1.5 | 20 |
Related posts:


Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


