CHAPTER 13 Treatment of Upper Eyelid Retraction: Internal Approach
For more than 30 years, I have preferred treating upper eyelid retraction secondary to thyroid ophthalmopathy with an internal rather than external approach. Excellent results, high patient satisfaction, and minimal need for secondary surgery lead to my bias toward this approach.
Upper eyelid retraction surgery occasionally is combined with retraction surgery of the lower eyelid, with or without lateral tarsorrhaphies (see Chapter 18). If there is minimal upper eyelid retraction, the surgery can be combined with an upper eyelid skin muscle-fat excision without eyelid reconstruction; if the retraction is moderate or severe, the external tissue excision is deferred to a second sitting since I am concerned that tightening of the skin might interfere with the results of the upper eyelid retraction surgery.
In this chapter, I describe a technique that Urist and I reported on in 1972, in which Müller’s muscle is excised and the levator aponeurosis is recessed from an internal approach.1 The procedure is performed with sensory but not motor anesthesia. The eyelid level is controlled intraoperatively while the patient is seated up on the operating table.
Anatomy
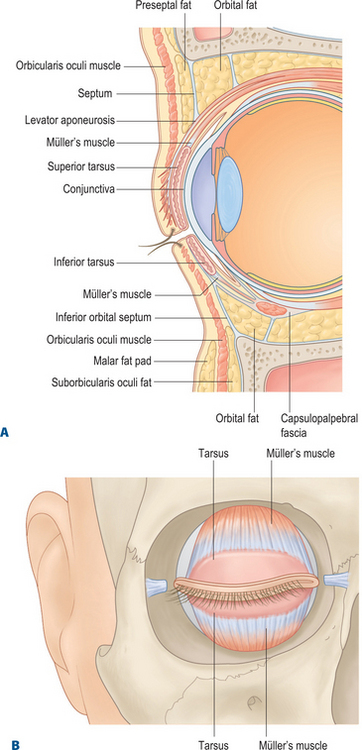
Müller’s muscle in the upper eyelid originates from the levator aponeurosis approximately 15 mm above the superior tarsal border and inserts onto the superior tarsal border (Fig. 13-1). This muscle spans the horizontal dimension of the eyelid, is firmly attached to conjunctiva on its posterior surface, and is loosely attached to the levator aponeurosis on its anterior surface. Müller’s muscle resembles other smooth muscle tissue and is approximately 1 mm thick.
Margin reflex distance-1
It is important to assess the upper eyelid levels with the margin reflex distance-1 (MRD1) measurement (see Chapter 3, Fig. 3-8).
Surgical technique
Anesthesia
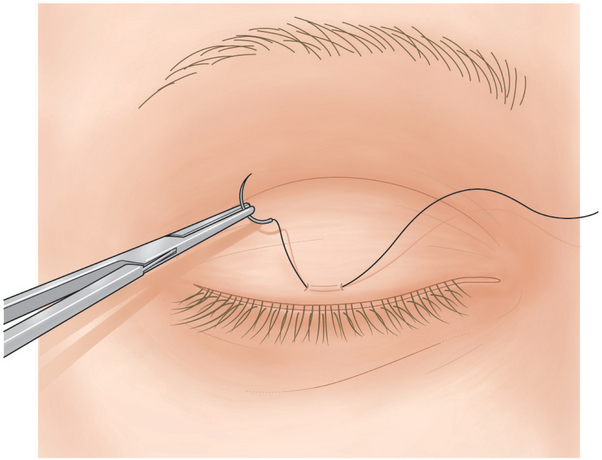
A 4-0 silk suture is placed in the center of the upper eyelid 2 mm above the eyelash line, through the skin, orbicularis muscle, and anterior tarsus (Fig. 13-2). Topical 0.5 percent tetracaine drops are applied to the eye, and a scleral lens is placed over the globe to protect it during surgery.
Conjunctival dissection
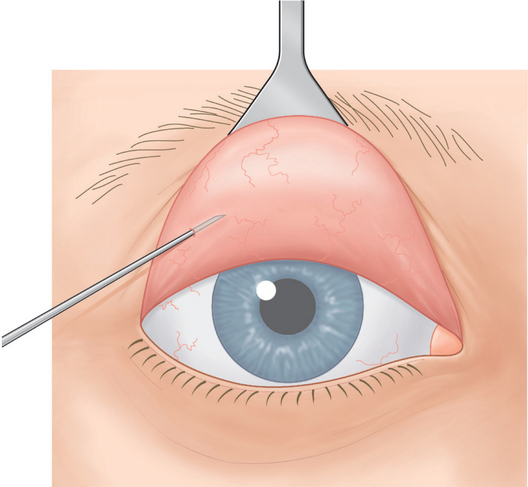
With a Desmarres retractor, the surgeon everts the upper eyelid to expose the superior palpebral conjunctiva. The upper palpebral conjunctiva is flooded with 0.5 percent tetracaine drops. Cotton-tipped applicators saturated with tetracaine also are rolled over the conjunctiva. Then, 0.25–0.5 ml of 2 percent lidocaine with epinephrine is injected subconjunctivally adjacent to the superior tarsal border over the entire width of the eyelid (Fig. 13-3).
Related posts:
 Upper Blepharoplasty Combined with Levator Aponeurosis Repair
Upper Blepharoplasty Combined with Levator Aponeurosis Repair
 Evaluation of the Cosmetic Oculoplastic Surgery Patient
Evaluation of the Cosmetic Oculoplastic Surgery Patient
 Brow Lift Techniques
Brow Lift Techniques
 Treatment of Lower Eyelid Retraction with Recession of Lower Lid Retractors and Placement of Hard-Palate or Allogeneic Dermal Matrix Spacer Grafts
Treatment of Lower Eyelid Retraction with Recession of Lower Lid Retractors and Placement of Hard-Palate or Allogeneic Dermal Matrix Spacer Grafts
 Eyelid and Facial Laser Skin Resurfacing
Eyelid and Facial Laser Skin Resurfacing
 Lower Blepharoplasty: Blending the Lid/Cheek Junction with Orbicularis Muscle and Lateral Retinacular Suspension
Lower Blepharoplasty: Blending the Lid/Cheek Junction with Orbicularis Muscle and Lateral Retinacular Suspension
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


