CHAPTER 7 Treatment of Upper Eyelid Dermatochalasis with Reconstruction of Upper Eyelid Crease: Skin-Muscle Flap Approach
I treat only about 10 percent of my patients with dermatochalasis (excess skin) and herniated orbital fat of the upper eyelid by performing an upper eyelid blepharoplasty with skin or skin-muscle resection alone. In 90 percent of patients, I perform a skin and orbicularis oculi muscle resection with or without fat removal, but with reconstruction of the eyelid crease.
Preparation for surgery
Surgical technique
Skin marking
A line is drawn with a methylene blue marking pen, beginning at the lateral canthus and extending in a horizontal direction of approximately 1 cm. This line marks the site of the lower lateral canthal incision. The site of the predetermined eyelid crease is then marked. When the surgeon is drawing the eyelid crease marks, the eyebrow must be elevated to reduce the excess upper eyelid skin fold and to make the upper eyelid skin taut and the lashes slightly everted. If this is not done, the crease may result in being much higher than desired because the skin is usually loose before it is marked.
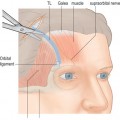
The temporal, central, and nasal marks are then connected and are extended with a line, which begins at the punctum and ends at the lateral canthus (Fig. 7-1A). The line sweeps laterally approximately 1 cm temporal to the lateral canthus in a slightly upward direction. There should be at least 5 mm of skin between this line and the line placed for the lower lateral incision.
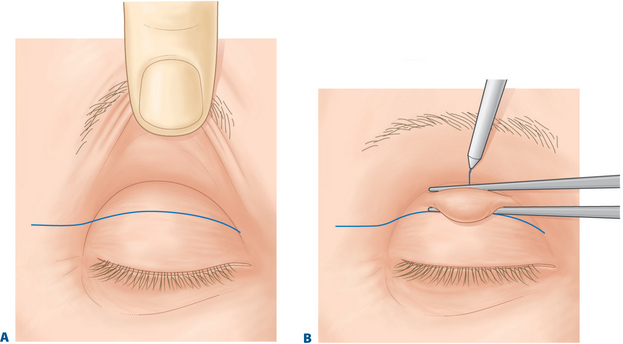
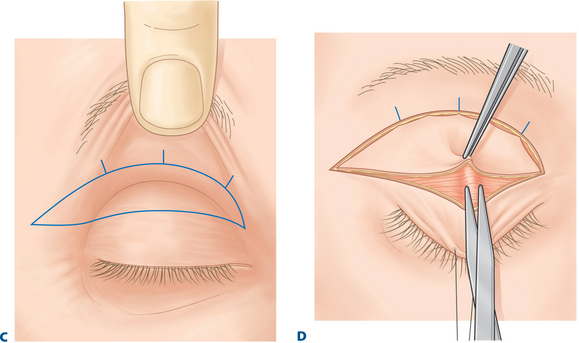
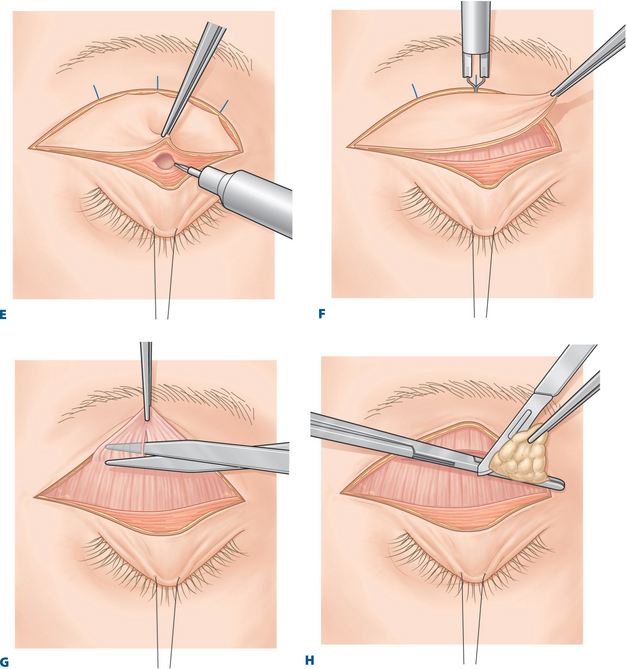
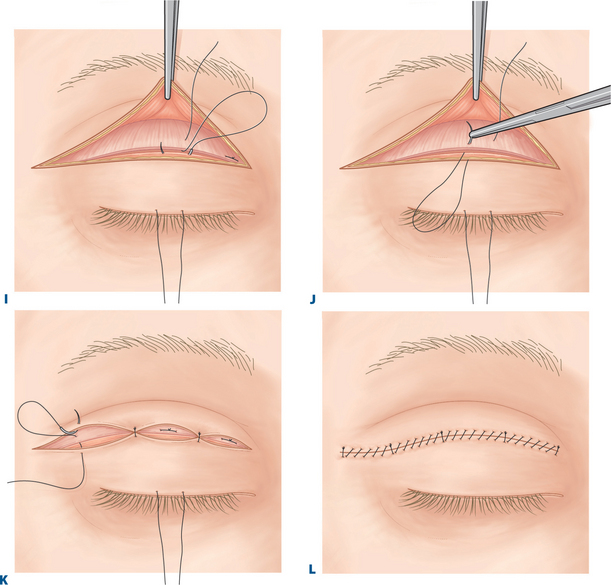
Figure 7-1 A, A line is drawn on the eyelid at the level of the eyelid crease.
D, A blunt Westcott scissors is used to make a buttonhole incision in the orbicularis oculi muscle.
E, The orbicularis oculi muscle along the lid crease incision is severed with a disposable cautery.
H, The nasal fat pocket is removed.
J, The 6-0 polyester fiber suture passes through the levator aponeurosis inferiorly to superiorly.
Related posts:
 Upper Blepharoplasty Combined with Levator Aponeurosis Repair
Upper Blepharoplasty Combined with Levator Aponeurosis Repair
 Brow Lift Techniques
Brow Lift Techniques
 Transconjunctival Approach to Resection of Lower Eyelid Herniated Orbital Fat
Transconjunctival Approach to Resection of Lower Eyelid Herniated Orbital Fat
 Treatment of Lower Eyelid Retraction with Recession of Lower Lid Retractors and Placement of Hard-Palate or Allogeneic Dermal Matrix Spacer Grafts
Treatment of Lower Eyelid Retraction with Recession of Lower Lid Retractors and Placement of Hard-Palate or Allogeneic Dermal Matrix Spacer Grafts
 Eyelid and Facial Laser Skin Resurfacing
Eyelid and Facial Laser Skin Resurfacing
 Lower Blepharoplasty: Blending the Lid/Cheek Junction with Orbicularis Muscle and Lateral Retinacular Suspension
Lower Blepharoplasty: Blending the Lid/Cheek Junction with Orbicularis Muscle and Lateral Retinacular Suspension
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


