A septal deformity with severe deviation of the septal L strut is seen in nearly every crooked or scoliotic nose. Unless the underlying septal deformity is properly diagnosed and treated, the nasal axis cannot be completely straightened. In addition, because standard septoplasty techniques often fail to adequately address severe L-strut deformities, extracorporeal septoplasty is often a prerequisite for straightening the crooked nose. This article presents a detailed explanation of the extracorporeal technique, as well as representative long-term clinical results showing the efficacy and durability of extracorporeal septoplasty. Extracorporeal septoplasty a safe and reliable method for straightening the severely deviated nose.
Key points
- •
Successful correction of the crooked nose requires a straight and sturdy L strut.
- •
Traditional septoplasty techniques are often ineffective at correcting deviation and deformities of the L strut.
- •
Contemporary rhinoplasty techniques made possible by the open rhinoplasty approach permit effective reconstruction of the deformed septal L strut.
- •
In severe cases, extracorporeal reconstruction in which the septal partition is removed from the nose, reconstructed, and then reimplanted, is necessary to achieve a strong, flat, and size-appropriate neoseptum and a straight nose.
Introduction
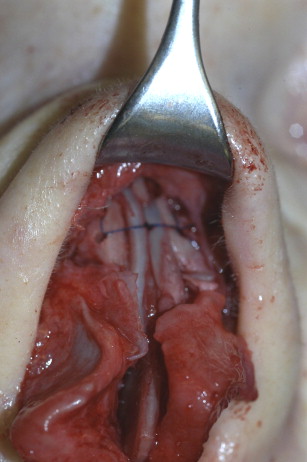
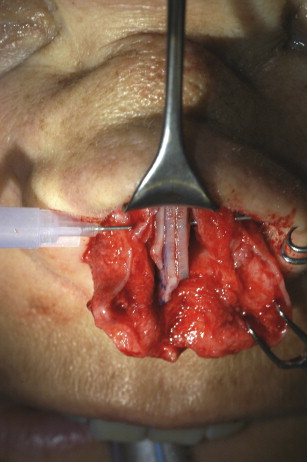
The idea of removing a severely deformed septum, reconstructing it on the table, and reimplanting the neoconstruct back into the nose was first published by King and Ashley in 1951. The concept of extracorporeal septal reconstruction was then revisited in the early 1990s to treat stubborn deformities of the anterior septal L strut. We have since refined the original technique to include en bloc removal of the bony-cartilaginous partition, creation of a flat and rigid L-strut replacement graft using autologous graft material (preferably salvaged from the septal partition), and secure fixation of the neoseptum to both the bony and cartilaginous skeletal framework. In the nearly 3 decades since we began performing extracorporeal septoplasty, much has changed with our technique. At present, we routinely perform extracorporeal septoplasty as part of a complete septorhinoplasty, including tip-plasty and/or dorsal hump reduction with full mobilization of the nasal bones. Although some surgeons regard extracorporeal reconstruction as unacceptable risk because of aggressive skeletal destabilization, particularly when extracorporeal septoplasty is performed in conjunction with complete nasal osteotomies, in our clinical experience, extracorporeal septal reconstruction performed as a stand-alone procedure or as part of a complete septorhinoplasty is a safe, effective, and reliable means for correcting severe L-strut deformities, and complications stemming from excessive destabilization have been rare. However, unlike our initial extracorporeal technique, we no longer use the closed rhinoplasty approach and now perform extracorporeal septoplasty exclusively through the external (open) rhinoplasty approach. The improved exposure associated with the open approach allows vastly improved surgical access, which in turn permits secure suture fixation of the neoseptum to the bony and cartilaginous skeletal framework. Although we previously sutured the neoseptum only to the upper lateral cartilages (ULCs), we now also suture the neoseptum directly to the nasal bones ( Fig. 1 ) and to the anterior nasal spine via small osseous drill holes ( Fig. 2 ). Often we also drill a sagittal groove in the nasal spine for improved stabilization of the inferior caudal septum, and when necessary the bony nasal spine is transected at its base, relocated to the sagittal midline, and reattached with microplates and microscrews in order to ensure accurate midline positioning of the columellar pedestal ( Fig. 3 ). Internal nasal valve patency is also enhanced using spreader grafts or spreader flaps in virtually every extracorporeal septoplasty, simultaneously enhancing both structural stability and nasal airway function.

Modification of the original extracorporeal septoplasty technique described herein has improved the efficacy of extracorporeal septoplasty and simultaneously reduced complications associated with treatment of the scoliotic nose. When performed correctly, the extracorporeal septoplasty, which is perhaps better termed extracorporeal septal reconstruction, is a reliable technique for straightening the twisted or deviated nose, and the modified technique has transformed the treatment of this previously challenging patient population.
Introduction
The idea of removing a severely deformed septum, reconstructing it on the table, and reimplanting the neoconstruct back into the nose was first published by King and Ashley in 1951. The concept of extracorporeal septal reconstruction was then revisited in the early 1990s to treat stubborn deformities of the anterior septal L strut. We have since refined the original technique to include en bloc removal of the bony-cartilaginous partition, creation of a flat and rigid L-strut replacement graft using autologous graft material (preferably salvaged from the septal partition), and secure fixation of the neoseptum to both the bony and cartilaginous skeletal framework. In the nearly 3 decades since we began performing extracorporeal septoplasty, much has changed with our technique. At present, we routinely perform extracorporeal septoplasty as part of a complete septorhinoplasty, including tip-plasty and/or dorsal hump reduction with full mobilization of the nasal bones. Although some surgeons regard extracorporeal reconstruction as unacceptable risk because of aggressive skeletal destabilization, particularly when extracorporeal septoplasty is performed in conjunction with complete nasal osteotomies, in our clinical experience, extracorporeal septal reconstruction performed as a stand-alone procedure or as part of a complete septorhinoplasty is a safe, effective, and reliable means for correcting severe L-strut deformities, and complications stemming from excessive destabilization have been rare. However, unlike our initial extracorporeal technique, we no longer use the closed rhinoplasty approach and now perform extracorporeal septoplasty exclusively through the external (open) rhinoplasty approach. The improved exposure associated with the open approach allows vastly improved surgical access, which in turn permits secure suture fixation of the neoseptum to the bony and cartilaginous skeletal framework. Although we previously sutured the neoseptum only to the upper lateral cartilages (ULCs), we now also suture the neoseptum directly to the nasal bones ( Fig. 1 ) and to the anterior nasal spine via small osseous drill holes ( Fig. 2 ). Often we also drill a sagittal groove in the nasal spine for improved stabilization of the inferior caudal septum, and when necessary the bony nasal spine is transected at its base, relocated to the sagittal midline, and reattached with microplates and microscrews in order to ensure accurate midline positioning of the columellar pedestal ( Fig. 3 ). Internal nasal valve patency is also enhanced using spreader grafts or spreader flaps in virtually every extracorporeal septoplasty, simultaneously enhancing both structural stability and nasal airway function.
Modification of the original extracorporeal septoplasty technique described herein has improved the efficacy of extracorporeal septoplasty and simultaneously reduced complications associated with treatment of the scoliotic nose. When performed correctly, the extracorporeal septoplasty, which is perhaps better termed extracorporeal septal reconstruction, is a reliable technique for straightening the twisted or deviated nose, and the modified technique has transformed the treatment of this previously challenging patient population.
Indications
Although the septum is the central element of the nasal framework, its importance is often overlooked in nasal surgery. Even now, many otolaryngologists are erroneously taught that a septoplasty is a suitable operation for the beginner and requires only 20 to 30 minutes to complete. However, not all septal deformities are amenable to correction with straightforward septoplasty techniques. Although septal deformities that are localized to the inferior/posterior aspect of the quadrangular septum can often be corrected with straightforward septoplasty techniques, these modest deformities cause only airway obstruction and do not produce deformities of the external nose. In contrast, complex septal deformities involving the outer septal L strut often produce both functional and cosmetic deformities, and these more severe septal deformities typically resist correction with traditional septoplasty techniques. Severe L-strut deformities are often impossible to eliminate with traditional septoplasty or rhinoplasty techniques. In contrast, not every septal deformity is responsible for the patient’s complaint of airway dysfunction, and a complete nasal examination, coupled with diagnostic testing, is necessary to localize alternative sources of airway dysfunction such as nasal valve collapse or turbinate hypertrophy. In addition, although a perfectly straight septal partition is seldom required for adequate nasal airway function, a perfectly flat and midline L-strut partition is a prerequisite for a straight, symmetric, and properly aligned outer nose. The importance of a straight septal L strut is often underappreciated by cosmetic nasal surgeons, who are primarily concerned with the aesthetic outcome and who often fail to recognize the contribution of the outer nasal septum to the cosmetic result. As a result, the preoperative assessment must seek to identify deformities within the septal L strut in order to devise a comprehensive and effective treatment plan.
According to the classification system described by Guyuron, septal deviations can be subdivided into 6 different types of anatomic deformity. C-shaped or S-shaped anterior-posterior septal deviations may lead to deformities of the dorsal L strut, whereas C-shaped or S-shaped cephalocaudal deviations can lead to deformities of the caudal (anterior) L strut. The remaining 2 classifications do not involve the L strut. Although some L-strut deformities can be treated effectively with traditional nonextracorporeal techniques, when properly executed the extracorporeal septal reconstruction can eliminate virtually any L-strut deformity and the extracorporeal technique remains the gold standard for severe anatomic derangements of the septal L strut.
Surgical technique
Dissection and en Bloc Removal of the Deformed Septum
In order to vasoconstrict the nasal mucosa, we prefer 2% ropivacaine, which is the only commercially available local anesthetic with intrinsic vasoconstrictive properties. For additional vasoconstriction the ropivacaine is mixed with epinephrine at a final concentration of 1:100,000. Following careful injection of the septal mucosa and the cutaneous incision lines, we obtain surgical access via the open (external) rhinoplasty approach. Because asymmetric scars are best avoided in the facial midline, we start with bilateral marginal incisions for dissecting the tip blindly, before we connect the marginal incisions with the transcolumellar incision, the upper membranous septum is dissected to expose the anterior septal angle, formed by the junction of the dorsal and caudal L struts. Once the anterior septal angle is identified, we elevate the mucoperichondrium with sharp-tipped scissors and begin blindly elevating tunnels along the dorsal septum at its junction with the ULCs. Once the septal/ULC junction has been denuded of mucosa, both ULCs are severed from the dorsal septum taking care not to injure the underlying nasal mucosa. A swivel-headed suction elevator is then used to extend the submucosal tunnels cranially beneath the nasal bones. In previously operated noses or in cases of severe anterior septal deformity, we have found that dissection is often easier when performed in an anterior-to-posterior direction using 2 parallel pairs of tunnels: one pair of tunnels along the dorsal septum and another pair just above the nasal floor. In the next step we consequently create separate inferior septal tunnels, starting at the piriform aperture, using a small periosteal elevator specifically designed for this purpose ( Fig. 4 ). In addition, both tunnels are gradually joined in an anterior-to-posterior direction until the mucoperichondrial/mucoperiosteal flaps are completely elevated on both sides of the septal partition.
In most cases, before removing the septal partition we create parallel medial osteotomy cuts using an electric drill fitted with a narrow Lindeman bur equipped with both side-cutting and end-cutting capacity ( Fig. 5 ). In addition to creating perfect parasagittal osteotomy cuts for a straight and symmetric bony infracture, the Lindeman bur also removes small amounts of bone to produce a slender open-roof deformity in order to facilitate adequate narrowing of wide or stubborn nasal bones following both transverse and lateral osteotomies. In addition, the Lindeman bur is also used to make a 45°downward diagonal cut across the perpendicular ethmoid plate in order to reduce the risk of inadvertent cribriform disruption when fracturing the vertical ethmoid bone. Inferiorly, the maxillary crest and vomer are cut horizontally (beginning immediately posterior to the incisive foramen) using a 5-mm chisel. A posterior vertical fracture is then created by pressing firmly against the posterior bony septum with the 5-mm chisel. Care is taken to release all soft tissue attachments before attempting en bloc removal of the septal partition.
Analysis and Correction of a Malpositioned Anterior Nasal Spine
The next step is the assessment of the anterior nasal spine (ANS). In many patients with a severely deformed septum, and in all patients with a unilateral cleft nose, the ANS is displaced from the midline prohibiting fixation of the caudal septum in the sagittal midline. Our treatment algorithm depends on both the extent of bony displacement and the width of the ANS. If there is only minor displacement and the ANS is sufficiently wide (and at least partly in the midline), it can be narrowed on the protruding side using a cylindric cutting drill so that the residual bone rests in the midline. Transverse drill holes are then created in the residual ANS and suture fixation is used to secure the reimplanted caudal L strut in the midline. However, when the ANS is completely displaced from the sagittal midline, we use the Lindeman bur to transect the ANS at its base, releasing the ANS from the premaxilla but leaving it pedicled anteriorly to the soft tissues. The ANS is then repositioned in the sagittal midline and reattached with an angled 4-hole microplate and two 3-mm to 5-mm microscrews (see Fig. 3 ). Because the ANS is no longer large enough to permit placement of transverse drill holes, the reimplanted caudal septum is usually sutured directly to the microplate for midline fixation.
Septal Reconstruction: Creation of a Neoseptum
The reconstruction of a straight neoseptum varies according to the septal deformity. In many cases, the caudal septum is severely deflected and must be excised. The remaining septum can usually be rotated by 90° such that the existing bony-cartilaginous (B-C) junction becomes the new dorsal septum. The desired length of the dorsal septum is predetermined using measurements from the native septum. Although straight, the B-C junction is usually thicker on one side, which necessitates either augmentation of the deficient side or thinning of the thickened side with a cylindrical bur. If the residual septum has a sufficiently large quadrangular cartilage, the septum can be cut approximately 5 mm below the B-C junction leaving a residual strip for use in augmentation of the deficient side or for use as a unilateral spreader graft, sometimes pedicled on perichondrium. As an alternative, spreader grafts can be fabricated from the resected portions of the deformed caudal septum or from surplus cartilage harvested away from the neo–L strut. However, when only crooked cartilage segments are available for spreader graft fabrication, the cylindrical drill can sometimes be used to eliminate thickened segments and produce a suitable spreader graft. Otherwise the deformed cartilage segments can be scored and splinted using perforated ethmoid bone grafts. Care must be taken to create as many drill holes as possible within the ethmoid bone so as to facilitate both suture fixation and optimal vascular and fibrous tissue ingrowth. When ethmoid bone is unavailable, bent segments of cartilage can be straightened using horizontal mattress sutures as described by Gruber and colleagues. In addition, in the severely deformed septum, multiple small flat segments can be harvested and splinted with perforated ethmoid bone or polydioxanone (PDS) plate to create a mosaiclike neo–L strut.
In the previously operated nose in which nearly all of the septal cartilage is absent but sufficient vomerine and/or ethmoid bone is available to create an L strut of appropriate size, we thin the donor bone where necessary and create as many drill holes as possible without jeopardizing structural stability. In addition to making fixation easier, multiple drill holes promote better revascularization and stabilization by the ingrowth of fibrous tissue. They also permit transfixion sutures, which are sometimes added for additional structural stability. If no cartilage or bone is available to create a stable and flat L strut, the entire neoseptal construct must be created from either bilateral conchal grafts or from costal cartilage.
Creation of a Neoseptum Entirely from Conchal Cartilage
When sufficient nasal graft material is unavailable to permit construction of a strong and straight L-shaped neoseptum, both conchal donor sites can be used for septal reconstruction. The concha is harvested as a single en bloc specimen from each ear, and the convex side of each graft is sutured back to back with its counterpart using several longitudinal rows of running suture. To facilitate suture placement, a modified Aiach clamp is used to immobilize the grafts in a flat and symmetric orientation ( Fig. 6 ). After suture fixation, the newly created sandwich graft remains flat and stabile, and the edges can be trimmed to create a smooth straight edge to form the L strut. When necessary, portions of the graft not contributing to the L strut can be excised and used for other purposes.