Treating the Narrow Midvault
Eric J. Culbertson
Jason Roostaeian
DEFINITION
The brow-tip dorsal aesthetic lines on frontal view are paired gentle curvilinear lines starting at the medial brow curving medially along the nasal bridge before transitioning laterally to the tip. This line can be disrupted by bony irregularities of the upper third of the nose, middle vault contour deformities in the middle third, and deviations of the tip or asymmetry of the lower lateral cartilages in the lower third. Restoration of this and other nasal aesthetic contours is key to achieving an optimal result following rhinoplasty (FIG 1A).1
ANATOMY
The middle vault is composed of the paired upper lateral cartilages, overlying soft tissue and skin, and underlying attached mucosa. Superiorly, the keystone area (also referred to as the K area) is the junction of the upper lateral cartilages with the nasal bones. Inferiorly in the scroll area, the upper and lower lateral cartilages are connected by loose areolar and fibrous attachments (FIG 2).
The internal nasal valve is defined by the caudal border of the upper lateral cartilage, the septum, the head of the inferior turbinate, and the piriform aperture. Nasal airway resistance accounts for more than 50% of total airway resistance during nasal breathing, and the internal nasal valve has the smallest cross-sectional area of the nasal airway. The normal angle between the septum and upper lateral cartilage is 10 to 15 degrees (FIG 3A). An angle below this range can contribute to nasal obstruction (FIG 3B).3
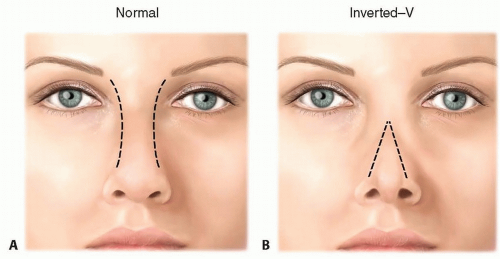 FIG 1 • Normal brow-tip aesthetics form paired curvilinear lines from the medial brow to the tip (A). Midvault narrowing can disrupt these lines and distort the aesthetics of the nose, with a visible inverted-V deformity (B). |
PATHOGENESIS
Midvault narrowing is a common sequela of rhinoplasty, particularly following dorsal hump reduction. Reduction of the cartilaginous component frequently disrupts the relation and attachments of the septum with the upper lateral cartilages, which form a single entity. Cartilage resection can result in an open roof deformity and allow collapse of the upper lateral cartilages, narrowing the internal valve angle and resulting in an inverted-V deformity and nasal obstruction. Often, this may not become apparent for months or years after surgery.
Patients at particular risk are those with short nasal bones, thin skin, weak cartilages, or a combination thereof.2
Scar contracture from tumor resection or trauma involving the lower portion of the nose may distort the internal nasal valve.
Facial paralysis may cause internal and external valve collapse through ptosis of the lateral nasal soft tissues and loss of muscle tone that normally prevents valve collapse, particularly on inspiration.
Weakening of the attachments between the upper and lower lateral cartilages with age may lead to senile tip ptosis that can also cause internal valve narrowing.
PATIENT HISTORY AND PHYSICAL FINDINGS
A detailed nasal history should be obtained, in particular to include a history of symptoms related to nasal obstruction, nasal allergies, prior nasal trauma, and nasal surgeries. Any patient aesthetic concerns and goals should be elicited and clearly defined.3,4
A complete external and internal nasal examination should be conducted in all patients.
Evaluate symmetry of the upper lateral cartilages. An inverted-V deformity may be present as a result of collapse of the upper lateral cartilages.
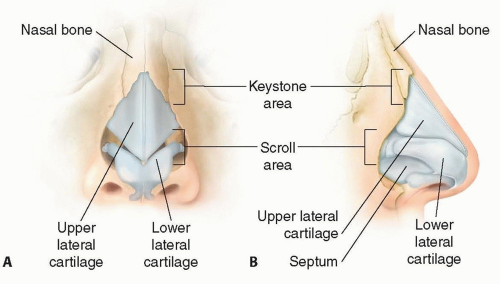
FIG 2 • A,B. Normal nasal anatomy.
Perform a Cottle maneuver, where the cheek immediately adjacent to the nasal sidewall is displaced laterally to assess for improvement in nasal airway obstruction with widening of the internal nasal valves. Gentle internal elevation of the upper lateral cartilages using a cotton-tipped applicator will also improve breathing in patients with midvault narrowing. Patency of the internal nasal valve during inspiration should also be assessed.
A nasal speculum is used to evaluate the septum for deformities and the inferior turbinates for hypertrophy.
Standardized photographs including frontal, lateral oblique, and basal views should be obtained in all patients.
IMAGING
Imaging is seldom required for diagnosis or treatment; however, supplemental testing can be performed to assess airway dynamics. Rhinomanometry measures pressure and flow during inspiration and expiration and provides a measure of airflow resistance and nasal patency. Acoustic rhinometry analyzes reflected sound waves directed through the nostrils and can be used to measure cross-sectional area and nasal volume to quantify nasal obstruction.5
SURGICAL MANAGEMENT
The primary objective is to correct any functional airway obstruction caused by narrowing of the internal nasal valve.
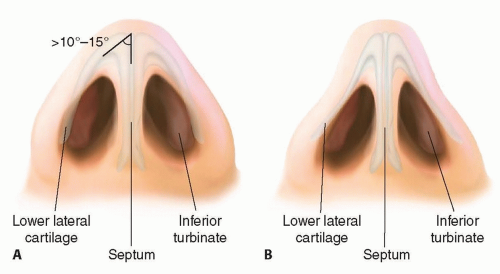
FIG 3 • Normal middle nasal vault anatomy is demonstrated. The normal angle between the septum and upper lateral cartilages is 10 to 15 degrees (A). A more acute angle may narrow the midvault and cause obstruction of the internal nasal valve (B).
Aesthetic concerns and goals for treatment discussed with the patient may also be addressed, particularly to restore symmetric and pleasing dorsal aesthetic lines.
The use of spreader grafts to reconstruct the roof of the middle nasal vault and open the internal nasal valve was first described by Jack Sheen, originally through an endonasal approach.2 Either an open or endonasal approach may be used for spreader graft placement. The use of the upper lateral cartilages as autospreader grafts or flaps, reducing the need to harvest cartilage grafts, was subsequently described.
Preoperative Planning
In planning the operative approach, it is important to carefully review the preoperative photos and establish clear goals of treatment with the patient. Consideration of previous operations, extent of previous nasal trauma, and involved structures and available septal and other potential cartilage grafts (ear, rib) should be taken into account. The patient should be informed of the possible need to harvest cartilage from these other donor sites such as the ear or rib.
Positioning
The patient is positioned supine on the operating table with arms tucked at the side.
An oral right angle endotracheal tube is used for intubation, and should extend inferiorly in the midline away from the nose, and secured without distorting the upper lip and nose.
Nasal hairs may be trimmed, if desired.
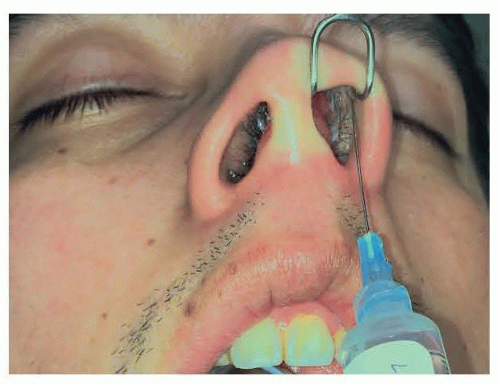
FIG 4 • Local anesthetic is injected into the nasal sidewalls, columella, and inside the nostril along the lower lateral cartilages.
Local anesthetic consisting of 1% lidocaine with 1:100 000 epinephrine is infiltrated into the nasal sidewalls and columella and inside the nostril along the lower lateral cartilages (FIG 4).Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree