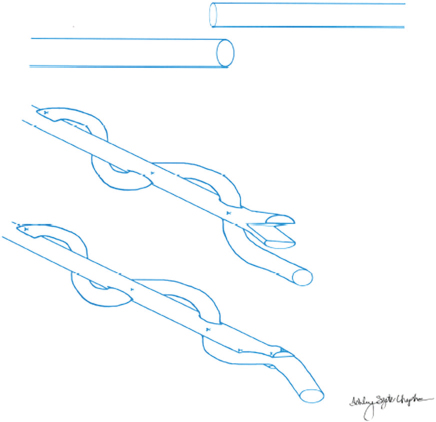
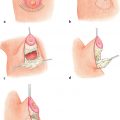
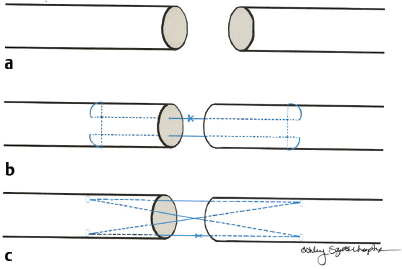
17 Traumatic Hand Injury Abstract Because specific trauma may vary, the chapter will provide an approach to the diagnosis and management of hand trauma using specific case examples, so that readers will feel confident addressing hand trauma that they may not have seen before. Keywords: hand trauma, hand therapy Six Key Points • Assessment of hand injuries includes a systematic assessment and catalogue of injured structures. • Identifying the injury/deformity is critical. • Early institution of hand therapy protocols is necessary for hand injuries. • The majority of postoperative hand-specific complications can be diagnosed by physical examination; imaging can be used as an adjunct. • Intraoperative complications include loss of vascularity, and vasospasm should be treated with papaverine or lidocaine. • Unrecognized injuries can lead to secondary deformities, such as a swan neck deformity after flexor digitorum superficialis rupture. A patient resents the injury in Fig. 17.1. 1. Describe what you see. A laceration between the A1 pulley at the palm and the insertion of the flexor digitorum superficialis on the middle phalanx, with loss of active flexion of the distal interphalangeal joint (IPJ) and proximal IPJ, is most consistent with a Zone 2 flexor tendon laceration, of both the flexor digitorum profundus and flexor digitorum superficialis tendon. 2. What do you do? Assuming that this is an isolated trauma and the patient has no other contraindications for surgical intervention, the ideal window to take the patient to the OR is within 72 hours. The patient should be consented for a primary tendon repair but be prepared for the possibility of a two-stage repair. 3. Describe your operative steps and explain how you repair the tendon. The operation is performed under general anesthesia or an axillary block, and a padded pneumatic tourniquet is placed on the arm. The original laceration is identified, and Bruner zigzag incisions are designed such that the points of the incisions are on the radial or ulnar aspect of the finger at the flexion creases. The neurovascular bundles are identified and retracted radially and ulnarly, and the tendon sheath is identified. The distal and the proximal stumps are identified. 4. You can’t see the proximal stump. What do you do? It is possible that the stump has retracted, depending on how flexed the finger was during the injury. The palm can be milked and this sometimes delivers the tendon. Fig. 17.2 Schematic of two-strand and four-strand core suture repairs for tendons. (a) The cut tendon edges. (b) The two-strand modified Kessler repair. (c) The four-strand cruciate repair. (Reproduced with permission of Ashley Szuter-Uncapher, Clinical Photographer.) If this does not work, a small incision can be made at the level of the A1 pulley and a small catheter such as a pediatric number 8 feeding tube can be fed through the sheath, attached to the tendons, to deliver the tendon. This technique is described by Sourmelis and McGrouther.1 5. You find the proximal stump this way. How do you repair the tendon? The tendon should be repaired with a four-strand core repair. Studies of sutures show that core suture strength is a function of three variables: type of suture, caliber of suture, and number of strands in the repair. A two-strand repair such as Kessler or modified Kessler is less strong than a four-strand repair such as a cruciate repair (Fig. 17.2), and an eight-strand repair is stronger than a four-strand repair.2 Ultimately, however, the bulk of the suture interferes with gliding. A four-strand repair, assuming that there is enough bulk of the tendon, is appropriate. Knots can be placed outside of the repair site.3 An epitendinous repair using a 6–0 Prolene will also increase strength. 6. What is your postoperative rehabilitation protocol? The patient sees a hand therapist within 5 days after surgery, and the postoperative splint is changed for a dorsal-blocking splint with the wrist in neutral, metacarpophalangeal joints (MCPJ) in 70 degrees of flexion, and IPJs in up to 10 degrees of flexion. An early active protocol is initiated in which the patient performs place-and-hold exercises for 3 minutes in the splint, followed by passive flexion and active extension in the splint. At 3 weeks, the splint can be removed for exercises, but remains in place otherwise. After 6 to 8 weeks, the splint can be removed in a controlled fashion. An alternative program is the Duran passive motion protocol, in which all exercises are performed in the splint. 7. After 3 months, the patient is not moving his finger that much. What do you do? The clinical question is whether the patient is not moving because of scar or rupture. An MRI may help elucidate the cause. If it is not clear from the MRI, the patient is consented for an exploration and a possible tenolysis versus a staged tendon reconstruction. 8. Describe a staged tendon reconstruction. A staged tendon reconstruction is performed if the tendons can’t be repaired primarily in the initial operation, for example, if there isn’t enough skin coverage or if there is too much of a gap. Once there is stable soft-tissue coverage, a Hunter rod is sutured distally and is brought proximally to the level of the carpal tunnel. It can either be left free or sutured to proximal tendon. The Hunter rod is left in place for 3 months, during which time a capsule forms around the rod. After 3 months, a tendon graft is placed.
Questions
Case 1
Plastic Surgery Key
Fastest Plastic Surgery & Dermatology Insight Engine