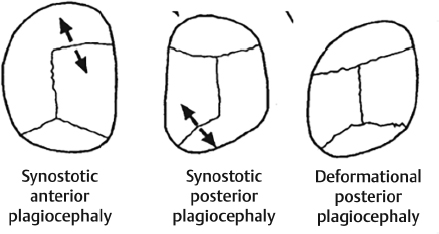
22 Craniosynostosis Syndromes Abstract This chapter will review craniofacial syndromes, with an emphasis on diagnosis and development of surgical management plans. The reader will be able to identify coexistent pathology and create timelines of surgical management and interventions. Keywords: craniosynostosis, plagiocephaly, surgical management Six Key Points • Children with craniofacial syndromes should be assessed for anomalies in other organ systems. • Assessment of the airway is the most important initial step. • Neurocognitive outcomes are always a consideration. • Timing of surgery is informed by osseous growth. • In airway compromise unresponsive to intervention, tracheostomy should be considered. • Distraction osteogenesis of the jaw should take into account tooth development. 1. What would you see in a photograph of a child with unilateral coronal craniosynostosis? The orbit in unilateral coronal craniosynostosis is differently shaped from one side to the other, with the eyebrow superiorly displaced on the affected side, and the nose and chin deviated toward the affected side. The shape of the orbit is called a harlequin deformity. The ear is anterior and superior on the affected side. 2. How do you distinguish this from nonsynostotic plagiocephaly? In nonsynostotic plagiocephaly, or deformational plagiocephaly, the appearance of the skull is a parallelogram (Fig. 22.1). 3. The mother calls and reports that the patient is tilting his head. What do you do? Children with unicoronal craniosynostosis can have head tilting because they have strabismus of the ipsilateral superior oblique muscle. I would have the patient see ophthalmology. 4. What operation do you offer the patient? For unicoronal craniosynostosis, a fronto-orbital advancement is recommended at the age 4 months. 5. Why 4 months? Why not when the child is older? There is some controversy in the literature. Some of the works by Marchac et al demonstrate that earlier intervention is prone to relapse, but later intervention (after 1 year of age) is associated with worse neuropsychological outcomes.1 6. The parents ask about cognitive outcomes. What do you tell them? There are several issues relating to neuropsychological outcomes. The first is how craniosynostosis compares to the nonsynostotic population. The second is how outcomes correlate to the timing of surgery, and the third is how the choice of operation influences the outcomes. Fig. 22.1 Comparison of unicoronal synostosis, lambdoid synostosis, and deformational plagiocephaly. (Adapted from Janis JE. Essentials of Plastic Surgery. 2nd ed. New York, NY: Thieme Medical Publishers; 2014) When compared to normative samples, nonsyndromic craniosynostosis is associated with cognitive, speech, and behavioral abnormalities.2 This is not predictive for any single child, but it does point to a need for longitudinal assessments and early intervention. Early intervention is associated with better neuropsychological outcomes when compared to later intervention (after 1 year of age).3 Some researchers have documented better neuropsychological outcomes from cranial vault remodeling compared to strip craniectomy for sagittal synostosis.4 7. What do you counsel the patients about complications? Complications of cranial vault remodeling include both aesthetic and neurosurgical complications. Aesthetic complications include poor cosmetic outcomes or relapse of the deformity, which has been shown to occur more with left-sided unicoronal craniosynostosis than with right-sided unicoronal craniosynostosis.5 Neurosurgical outcomes include dural leaks, sagittal sinus injury that may lead to venous infarction, increased intracranial pressure, subdural hemorrhage, and increased intracranial pressure.
Questions
Case 1
Related posts:



Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


