| Cosmetically displeasing lower eyelid fat prolapse with dermatochalasis |
| Functionally, when glasses rest upon excessive lower eyelid fat prolapse and causes lower eyelid ectropion |
| Prior facial surgery or trauma |
| Dry eye symptoms |
| Prior refractive surgery |
| Degree of dermatochalasis and fat prolapse |
| History of prior fillers to lower eyelid |
| Presence of midfacial ptosis |
| Presence of double convex deformity of lower eyelid |
| Presence of lower eyelid laxity or other eyelid malpositions |
Introduction
Transcutaneous lower blepharoplasty may be considered when addressing cosmetic lower eyelid fat prolapse with associated lower eyelid rhytids. When lower eyelid fat prolapse is the primary concern, the transconjunctival approach, as discussed in Chapter 9 , is a more appropriate choice.
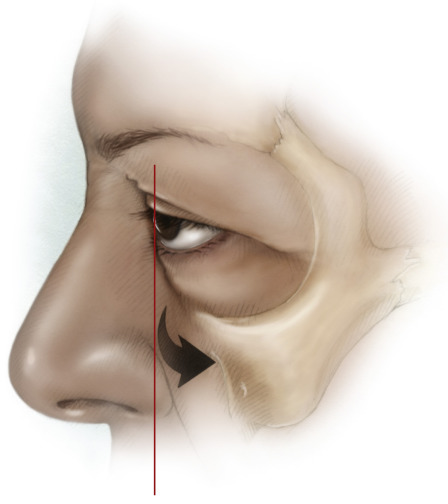
The preoperative evaluation should focus on aesthetic changes due to fat prolapse and skin redundancy as well as the contour changes of the lower eyelid and midfacial junction. Functional changes such as lower eyelid laxity, eyelid retraction, lagophthalmos and blink dynamics should be evaluated and addressed at the time of surgery. Patients with a prior history of blepharoplasty should be evaluated for eyelid retraction and eyelid closure and treatment should be directed at correction of these malpositions prior to blepharoplasty ( Chapter 34 , Chapter 35 , Chapter 36 ). Dry eye and tear film status should be determined and treated prior to surgery as well. Patients who have had keratorefractive surgery should have a careful evaluation for dry eye as this may worsen after blepharoplasty. Patients with a negative vector in which maxillary hypoplasia and a prominent globe are present are at high risk of lower eyelid retraction with transcutaneous lower blepharoplasty ( Figure 10.1 ) and are more appropriate for the transconjunctival approach ( Chapter 9 ). Photo documentation is essential and should be performed in the frontal plane, three-quarter, and side views to demonstrate changes after surgery.
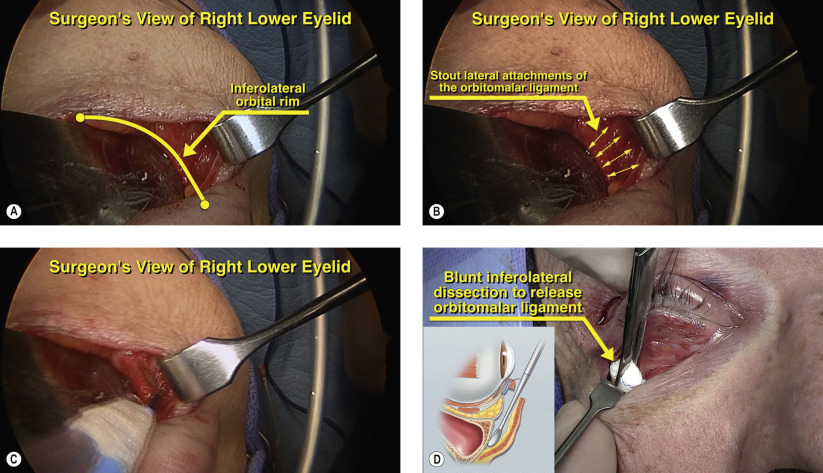
Several adjunctive procedures can be performed during transcutaneous lower blepharoplasty. Redraping of fat pedicles can address the double convex deformity of the lower eyelid ( Chapter 9 ). Judicious lower eyelid tightening, conservative skin removal and suborbicularis oculi fat lifting (orbitomalar suspension) at the time of surgery can minimize the risk of lower eyelid retraction and lagophthalmos. We routinely perform orbitomalar suspension on all cases of transcutaneous lower blepharoplasty to lessen the risk of lower eyelid malpositions as well as for the aesthetic benefits to the midface.
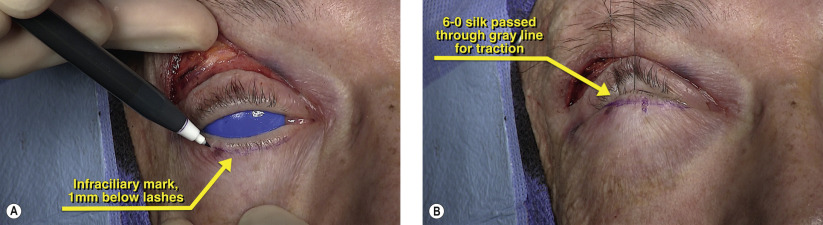
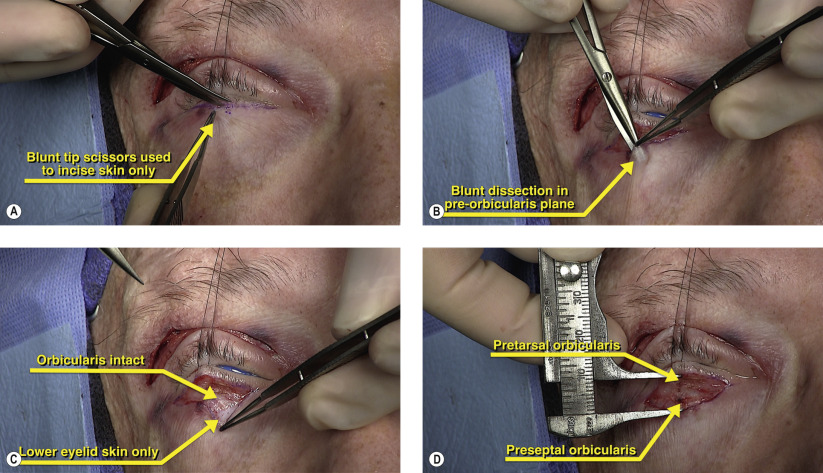
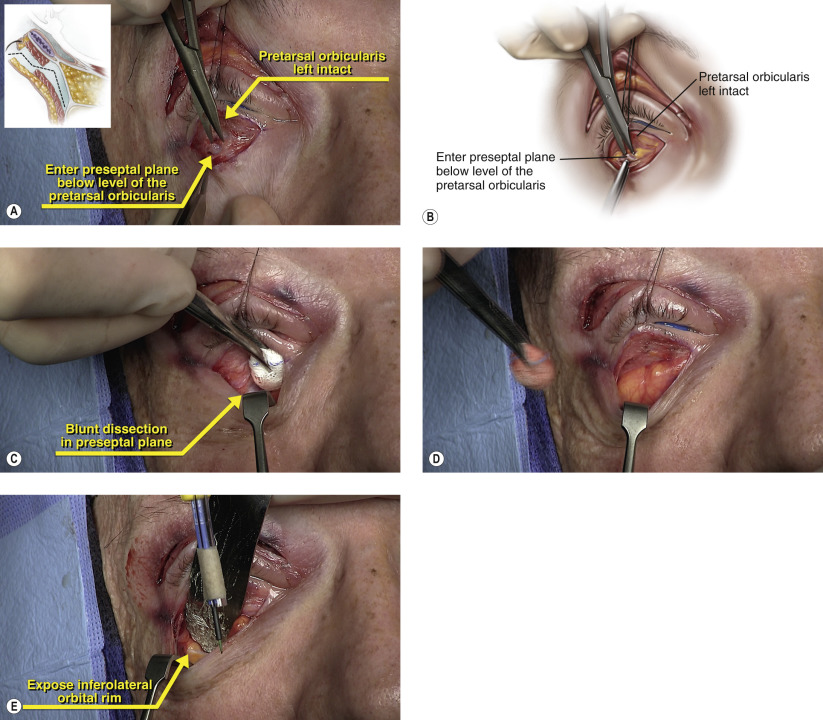
Surgical Technique
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


