CHAPTER 14 Transconjunctival Approach to Resection of Lower Eyelid Herniated Orbital Fat
The transconjunctival approach to removal of herniated orbital fat is the preferred method of treatment in patients who have only herniated orbital fat with minimal or no evidence of dermatochalasis (excess skin) and no hypertrophic orbicularis oculi muscle. This technique is also especially advantageous for:
If there is horizontal lower eyelid laxity, this procedure can be easily combined with a horizontal eyelid tightening through a tarsal strip procedure (see Chapter 1).
A contraindication to this procedure is with patients with minimal lower eyelid fat, inferior orbital rim or nasojugal hollowing and depression. In these patients, fat repositioning or cheek–midface lifting are indicated (Chapters 17 and 19).
Surgical technique
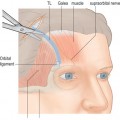
A Colorado needle or disposable cautery (Solan Accu-Temp, Xomed Surgical Products, Jacksonville, FL) is applied to the inferior palpebral conjunctiva. The Colorado needle or cautery are used to cut conjunctiva from the medial to temporal end of the eyelid halfway between the inferior palpebral fornix and the inferior tarsal border (Fig. 14-1). The surgeon grasps the inferior edge of the severed palpebral conjunctiva while the assistant grasps the adjacent, more superior edge with forceps and the assistant pulls the Desmarres retractor downward (Fig. 14-2
Related posts:
 Upper Blepharoplasty Combined with Levator Aponeurosis Repair
Upper Blepharoplasty Combined with Levator Aponeurosis Repair
 Evaluation of the Cosmetic Oculoplastic Surgery Patient
Evaluation of the Cosmetic Oculoplastic Surgery Patient
 Brow Lift Techniques
Brow Lift Techniques
 Treatment of Lower Eyelid Retraction with Recession of Lower Lid Retractors and Placement of Hard-Palate or Allogeneic Dermal Matrix Spacer Grafts
Treatment of Lower Eyelid Retraction with Recession of Lower Lid Retractors and Placement of Hard-Palate or Allogeneic Dermal Matrix Spacer Grafts
 Eyelid and Facial Laser Skin Resurfacing
Eyelid and Facial Laser Skin Resurfacing
 Lower Blepharoplasty: Blending the Lid/Cheek Junction with Orbicularis Muscle and Lateral Retinacular Suspension
Lower Blepharoplasty: Blending the Lid/Cheek Junction with Orbicularis Muscle and Lateral Retinacular Suspension
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


