Transconjunctival Approach to Resection and/or Repositioning of Lower Eyelid Herniated Orbital Fat
Allen Putterman
DEFINITION
This procedure is undertaken to treat baggy lower eyelids and inferior orbital rim hollowing.
ANATOMY
Pertinent anatomic structures are the lower eyelid conjunctiva, Müller muscle, capsulopalpebral fascia, orbital fat, and orbital septum (FIG 1).
There are three distinct lower eyelid orbital fat pads (nasally, centrally, and temporally).
The nasal and central fat pads are divided by the inferior oblique muscle, and the central and temporal fat pads are separated by the temporozygomatic ligament.
There may be a second temporal fat pad.1
PATIENT HISTORY AND PHYSICAL FINDINGS
Patients note fullness and bagginess of their lower eyelids. Some patients also notice a hollowing appearance in the inferior orbital rim area.
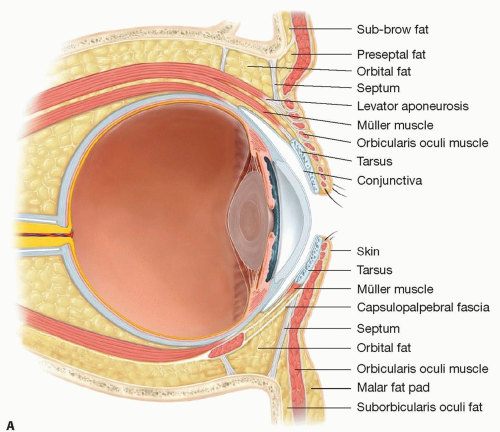
FIG 1 • Eyelid anatomy.
This technique is also especially advantageous for:
Younger patients with large amounts of herniated orbital fat
Patients who have had previous blepharoplasties and for whom an external approach might lead to eyelid retraction or ectropion
Fat repositioning is advocated for patients with inferior orbital rim hollowness.
SURGICAL MANAGEMENT
The transconjunctival approach to removal of herniated orbital fat is the preferred method of treatment in patients who have only herniated orbital fat with minimal or no evidence of dermatochalasis (excess skin) and no hypertrophic orbicularis oculi muscle.
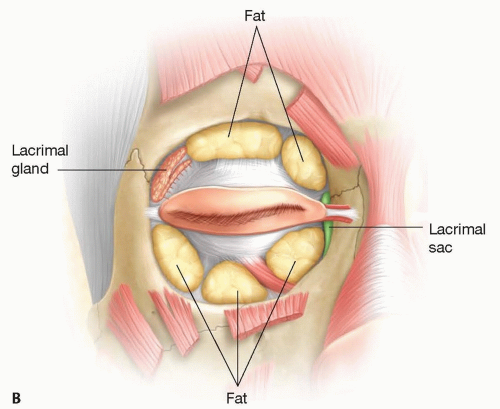 FIG 1 (Continued) |
TECHNIQUES
▪ Anesthesia and Eye Preparation
Two percent lidocaine (Xylocaine) with 1:100 000 epinephrine is injected subcutaneously at the center of the lower eyelid just beneath the lashes.
An additional anesthetic agent is injected into each fat pad.
To inject the anesthetic into the nasal, central, or temporal fat pad, the surgeon inserts a 25-gauge, 0.8-cm needle just above the inferior orbital rim and directs it downward slightly until it penetrates its entire length (0.8 cm).
The barrel of the syringe is withdrawn to make sure that no blood vessel has been entered and approximately 0.5 mL of the agent is injected into each of the three fat pads.
Topical tetracaine is instilled over the eye, and a scleral lens is placed over the eye to protect it.
A 4-0 black silk traction suture is placed through the skin, orbicularis muscle, and superficial fascia at the center of the eyelid. The surgeon pulls the eyelid downward with a traction suture as the assistant everts the lower eyelid over a small Desmarres retractor to expose the inferior palpebral conjunctiva.
Additional anesthetic is injected subconjunctivally over the inferior palpebral conjunctiva across the eyelid.
TECHNIQUES
▪ Isolating the Eyelid Retractors
A Colorado needle is used to cut the conjunctiva from the medial to temporal end of the eyelid halfway between the inferior palpebral fornix and the inferior tarsal border (TECH FIG 1A).
The surgeon grasps the inferior edge of the severed palpebral conjunctiva, while the assistants grasps the adjacent, more superior edge with forceps, and the assistant pulls the Desmarres retractors downward (TECH FIG 1B).
The two forceps are pulled apart.
Further dissection with the Colorado needle is carried out through the Müller muscle, and capsulopalpebral fascia until fat is seen.
A 4-0 black silk double-armed suture is passed through the inferior edge of the conjunctiva, the Müller muscle, and the capsulopalpebral fascia, and the suture arms are pulled upward and clamped to the drape (TECH FIG 1C).
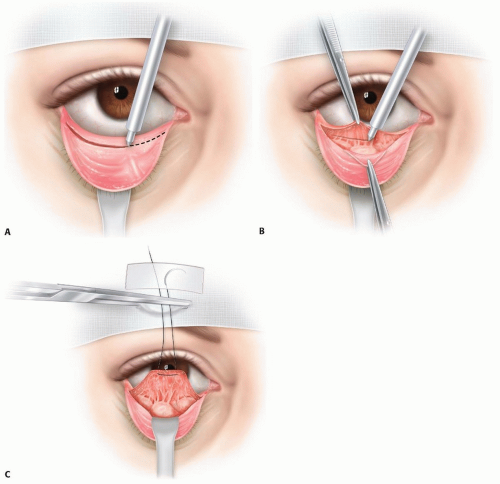 TECH FIG 1 • A. A Colorado needle is applied to the inferior palpebral conjunctiva halfway between the fornix and the inferior tarsal border and is used to sever the conjunctiva from medial to temporal end of the eyelid. B. With forceps, the surgeon and surgeon’s assistant grasp the inferior and superior edges, respectively, of the severed palpebral conjunctiva to facilitate dissection of the Müller muscle and capsulopalpebral fascia with the Colorado needle. C. A 4-0 double-armed black silk suture is placed through the inferior edge of the conjunctiva, Müller muscle, and capsulopalpebral fascia and is pulled upward and clamped and taped to the drapes. |
TECHNIQUES
▪ Excision of Orbital Fat
A small Desmarres retractor is placed over the lower eyelid and is pulled downward and outward to expose the orbital fat.Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree