The introduction of liposuction in the 1980s permanently altered the landscape of body contour surgery. The abdomen became a ‘‘group’’ of contour procedures that were referred to as the abdominolipoplasty system of classification and treatment (Types I-IV). This article describes a full (Type IV) abdominoplasty with or without liposuction is performed. When extensive abdominal liposuction is performed in conjunction with a full abdominoplasty, it is also known as lipoabdominoplasty. The article also describes 10 “special situations” in the abdominoplasty population.
The modern history of abdominoplasty can be traced to the late 1960s and 1970s, and was marked by acceptance of abdominoplasty as a bona fide aesthetic procedure with excision of the pannus, tightening of the underlying musculature, numerous incision designs, recognition of complications, and performing it in conjunction with other cosmetic (eg, breast reduction, breast augmentation, and so forth) and noncosmetic procedures (eg, hysterectomy, cholecystectomy, and so forth).
The introduction of liposuction in the 1980s dramatically and permanently altered the landscape of body contour surgery. Liposuction as a sole contouring procedure or in combination with excisional procedures represented the greatest advance in body contour surgery, even to date. In many instances incisions were shortened and patients heretofore not considered feasible as candidates were able to be treated. Indeed the abdomen became a “group” of contour procedures that were referred to as the abdominolipoplasty system of classification and treatment. This group included liposuction alone (type I), mini abdominoplasty (type II), modified abdominoplasty (type III) (type II and III are considered limited abdominoplasties), and a full standard abdominoplasty (type IV) with or without liposuction ( Fig. 1 ).
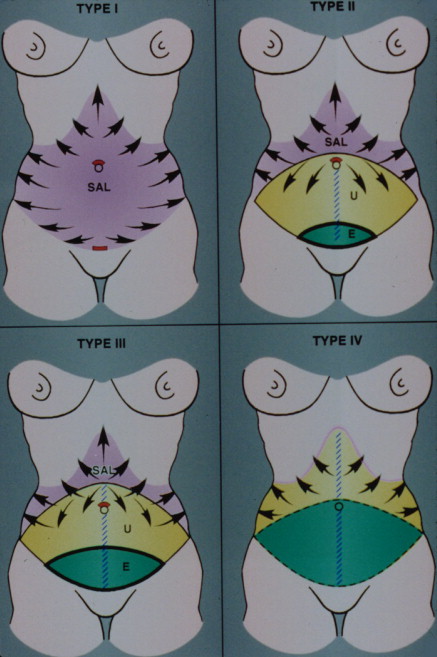
Extensive abdominal liposuction in conjunction with a full (type IV) abdominoplasty is known as lipoabdominoplasty, and is currently receiving renewed interest. Lipoabdominoplasty has also been referred to by various other nomenclatures such as suction-assisted abdominoplasty, abdominolipoplasty or marriage abdominoplasty. This article describes a standard abdominoplasty without or with liposuction (lipoabdominoplasty).
In the 1990s, with the increase in popularity of laparoscopic and arthroscopic procedures, attempts were made to perform abdominoplasty endoscopically. These procedures met with technical difficulties, a lack of refinement in instrumentation and, more significantly, the inability to address remaining excess skin, which often appears greater than anticipated after the rectus muscle is plicated. If applicable these techniques are most likely to be useful in males. It is this excess skin that must be excised that is ultimately the rate-limiting factor in the surgeon’s ability to shorten any abdominal incision. Unlike, for example, the face, where incisions can successfully be shortened while still removing the amount of skin necessary, in the abdomen as more skin needs to be removed the incision must be made longer.
The turn of the twenty-first century heralded the increase in bariatric surgery and subsequently an emerging field of bariatric plastic surgery. Abdominal contour surgery is the cornerstone of the numerous extensive excisional procedures undergone by patients with massive weight loss. It is interesting, then, that plastic surgery has gone full circle in less than a generation, from small incisional stab wounds for liposuction-dominated procedures to extensive lengthy incisions now deemed necessary for these large excisional procedures. In terms of abdominal liposuction, recent interest is now focusing on the benefits of laser-assisted liposuction (and the various wavelengths), and its role in facilitating fat removal and the unknown potential for skin tightening.
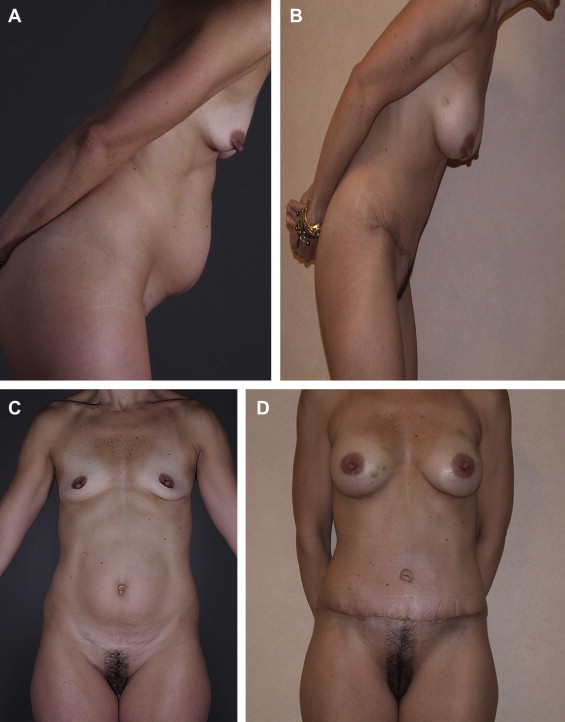
This article focuses on the most commonly encountered abdominoplasty scenario of the postpartum abdomen that manifests itself as loose, damaged, excess skin; widening (bony) pelvic girth; rectus muscle diastasis and stretching; alteration in the location of fatty deposits, umbilical hernias, and altered appearance of the mons pubis (with distortion, widening, and ptosis) ( Fig. 2 ). Emphasis is on technique. In addition 10 “special situations” encountered in the abdominoplasty population (eg, the scarred abdomen) are discussed. These often inevitable and irreversible changes of pregnancy continue to plague the physically fit, health-conscious baby-boomer generation accustomed to obtaining optimal goals, personally, professionally, and physically. Maintaining their youthful physique, fashions, and appeal, particularly in an environment that more than ever idealizes slimness, youthfulness, and vitality, along with the current trend of low-cut clothing (creating the ubiquitous “muffin top” appearance in pants) is a priority for these patients. Indeed people have a tendency to perceive their level of fitness or ideal weight (and the necessity to diet or exercise) by the appearance of their abdomen and flanks. In some it even acts as a surrogate marker for the aging process.
Related posts:
 Anatomic Considerations in Abdominoplasty
Anatomic Considerations in Abdominoplasty
 Editorial Comment on “Traditional Abdominoplasty”
Editorial Comment on “ SAFECircumferential Liposuction with Abdominoplasty”
Editorial Comment on “Traditional Abdominoplasty”
Editorial Comment on “ SAFECircumferential Liposuction with Abdominoplasty”
 SAFECircumferential Liposuction with Abdominoplasty
Editorial Comment on “Concepts on Correction of the Musculoaponeurotic Layer in Abdominoplasty”
Revision Abdominoplasty and Proper Umbilical Positioning
SAFECircumferential Liposuction with Abdominoplasty
Editorial Comment on “Concepts on Correction of the Musculoaponeurotic Layer in Abdominoplasty”
Revision Abdominoplasty and Proper Umbilical Positioning
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


