Knowledge of abdominal anatomy is key to achieving optimal results in abdominoplasty. With adequate knowledge of the anatomy, the surgeon can tailor his or her techniques to fit the needs of the patient while still maximizing the blood supply to the abdominal flaps and minimizing complications.
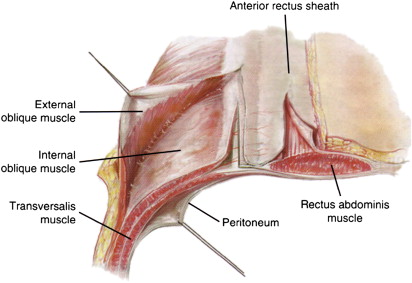
Successful abdominoplasty depends on knowledge and understanding of abdominal anatomy. Skin resections must be planned with to respect blood supply to the abdominal flap. Abdominal fat must be treated appropriately. The umbilicus must be handled so that its blood supply is maintained. Furthermore, the surgeon should be sure to preserve the blood supply to the remaining flap and consider liposuction or previous surgeries. The abdominal wall is composed of 6 distinct soft tissue layers: skin, subcutaneous fat, subscarpal fat, anterior rectus sheath, muscle, and posterior rectus fascia ( Fig. 1 ). The anatomy most relevant to planning and execution of successful abdominoplasty includes understanding abdominal landmarks, muscle and fascial anatomy, zones of adherence, and anatomy of the nerve supply to the abdominal wall, as well as blood supply to the remaining cutaneous flaps, fat, and umbilicus.
Anatomy
Anatomic Landmarks
The abdomen spans the area between the costal margin, midaxillary line, iliac crest, and symphysis pubis. The anterior and lateral contours of the abdominal wall, as well as the position of the umbilicus, are important landmarks that must be respected. The umbilicus is midline and is generally located at the level of the superior iliac crest. The umbilicus is normally located 14 cm above the pubic symphysis and 10 cm above the pubic hair. Checking these landmarks is helpful to ensure that the umbilicus is positioned appropriately postoperatively. The surgeon should also consider that the female abdomen has a more hourglass shape and is wider at the hips compared with the male abdomen that continues to narrow at the hips.
Muscle and Fascia Anatomy
The abdominal wall is composed of 4 paired muscle groups: the rectus abdominis, external oblique, internal oblique, and transversalis ( Fig. 2 ). In addition to flexion and rotation of the trunk, the abdominal muscles support the abdominal contents and assist in breathing. The midline of the abdomen is marked by a dense confluence of fascia known as the linea alba. Patients with a history of pregnancy or previous morbid obesity will frequently have a wider diastasis. The term abdominal diastasis refers to weakening and spreading of the midline fascia at the linea alba without the formation of a true hernia. In these cases aggressive plication may be used to improve and further flatten the abdomen and correct the diastasis.
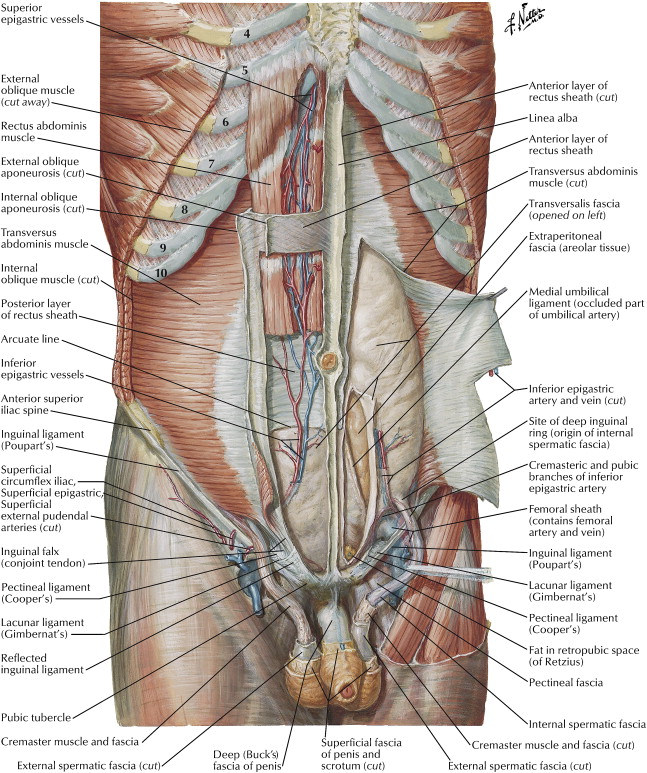
The paired rectus muscles are located on either side of the linea alba. The origin of the rectus abdominis muscle is the fifth, sixth, and seventh costal cartilages, costoxiphoid ligaments, and xiphoid process. The insertion of the rectus abdominis muscle is the crest of the pubis, pubic tubercle, and front of symphysis pubis. There are several horizontal inscriptions located on each rectus muscle. These condensations of fascia improve the mechanical advantage of the rectus muscle. The paired semilunar lines mark the lateral border of the rectus abdominis muscles. These vertical landmarks correspond to the aponeurosis of the external oblique, internal oblique, and transversus abdominis muscles. The aponeurotic portions of the oblique and transversus abdominis muscles surround the rectus abdominis muscles and join in the midline to form the linea alba.
The arcuate line is a horizontal transition point where the rectus fascia composition is different. Above the arcuate line the internal oblique fascia splits and part of the internal oblique fascia joins the external oblique to form the anterior rectus fascia. The other portion joins the aponeurosis of the transversus abdominis to form the posterior rectus sheath. Below the arcuate line, all 3 muscle aponeuroses pass anterior to the rectus abdominis muscle, leaving only preperitoneal fat between the rectus muscle and the underlying peritoneum.
The superficial and deep layers of fat in the abdominal wall are divided by Scarpa’s fascia. Scarpa’s fascia is a landmark dividing the better vascularized superficial fat from the less dense and less well vascularized deep fat. In addition, Scarpa’s fascia can be sutured to take tension off of the skin incisions. Suturing of Scarpa’s fascia may help achieve a fine line scar and limit scar migration.
Zones of Adherence
An understanding of the abdominal zones of adherence will facilitate appropriate design of flaps and prevent scar migration. There are zones of adherence located in the lower inguinal regions bilaterally and one centrally just above the mons pubis. The central zone may be less adherent in some individuals. These zones of adherence of the abdomen are important to prevent migration of abdominoplasty scars. Many advocate a deep layer of sutures using Scarpa’s fascia to facilitate anchoring at these zones of adherence. Note that there are also zones of adherence bilaterally between the hip and lateral thigh fat deposits as well as a zone of adherence overlying the spine. These latter zones are important particularly when abdominoplasty is combined with circumferential procedures. The zones of adherence are often most evident in patients with massive weight loss.
Nerve Anatomy
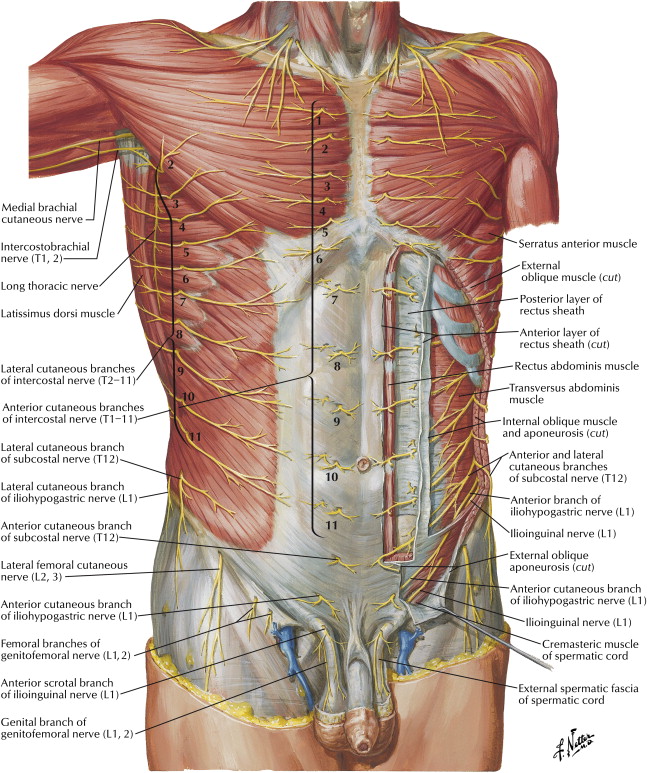
The cutaneous sensation to the abdominal wall is provided by the lateral cutaneous and anterior cutaneous branches of intercostal nerves T7 through T12 ( Fig. 3 ). These nerves typically perforate the intercostal muscles at the midaxillary line to travel within the subcutaneous plane. Therefore, nerves to the remaining skin flap are typically preserved in abdominoplasty. Also, consider the ilioinguinal and iliohypogastric nerves during abdominoplasty. Although they do not innervate the abdomen proper, they can be disrupted particularly with dissection in the lateral abdomen, resulting in sensory deficits in the medial thigh and groin.
Blood supply of the abdominal wall
An understanding of the abdominal blood supply is crucial to avoiding ischemic complications in abdominoplasty. One must consider not only the native blood supply but also the blood supply to the flaps after undermining and flap resection. The blood supply to the abdomen comes from numerous major arteries of the thorax and pelvic region ( Fig. 4 ). The anastomotic interconnections of these arteries are important for the abdominal flap to survive even when part of the blood supply has been disrupted by flap undermining during dissection. The blood supply of the abdomen can be divided into one that is superior-lateral in origin and one that is inferior in origin.
Related posts:
 Editorial Comment on “Traditional Abdominoplasty”
Editorial Comment on “Traditional Abdominoplasty”
 Traditional Abdominoplasty
Editorial Comment on “ SAFECircumferential Liposuction with Abdominoplasty”
Traditional Abdominoplasty
Editorial Comment on “ SAFECircumferential Liposuction with Abdominoplasty”
 SAFECircumferential Liposuction with Abdominoplasty
Editorial Comment on “Concepts on Correction of the Musculoaponeurotic Layer in Abdominoplasty”
Revision Abdominoplasty and Proper Umbilical Positioning
SAFECircumferential Liposuction with Abdominoplasty
Editorial Comment on “Concepts on Correction of the Musculoaponeurotic Layer in Abdominoplasty”
Revision Abdominoplasty and Proper Umbilical Positioning
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


