The SAFE Lipo technique allows for safe, consistent liposuction that does not damage flap blood supply and is easily taught to, and reproducible by, other surgeons. The fat separation used in the SAFE Lipo technique is performed without suction, which prevents suction avulsion injury to blood vessels by the cannula. Blood vessels then remain intact while free, separated fat is aspirated with small diameter cannulas.
The author performs circumferential liposuction of the trunk with abdominoplasty, using a “SAFE” (Separation, Aspiration, and Fat Equalization) liposuction technique designed to minimize vascular damage and contour deformities while maximizing fat removal and flap viability.
Patient selection
Healthy patients with a body mass index (BMI; weight in kilograms divided by height in meters squared) of less than 30 are the best candidates for circumferential liposuction of the trunk with abdominoplasty. In general, patients with BMIs of greater than 32 do not realize the full benefits of the limited amount of liposuction that can be performed safely with abdominoplasty. Similarly, these patients usually tolerate only a limited diastasis repair given their usual preponderance of intra-abdominal fat, further limiting the reduction of the waistline. Patients with a BMI of greater than 30 are counseled to lose weight before undergoing truncal contouring, to maximize results. In consideration of truncal contouring in women, most patients seek a more curvaceous and proportional outline of the waist and hip region. Excess fat, loose skin, and abdominal laxity all play important roles in choosing the best procedure for each patient. Consideration is first given to the amount of excess subcutaneous fat of the circumferential trunk, which is to be treated by liposuction. Skin excess and abdominal laxity are then assessed, and if present in sufficient amounts, mini-abdominoplasty or abdominoplasty is added to the treatment plan.
General Contraindications to SAFELipo Circumferential Liposuction with Abdominoplasty
As in any abdominoplasty procedure, the presence of a supraumbilical incision that cannot be removed with the excision of the pannus poses a significant risk to the vascularity of the abdominoplasty flap. In the presence of a scar that remains in the flap, a more conservative skin undermining is performed, usually limiting the continuous undermining to the area of diastasis repair, with conservative, discontinuous undermining to minimize skin irregularities, with care taken not to dissect beyond the scar. The SAFE liposuction technique is unaltered.
Patients with a history of mesotherapy or various forms of injection lipolysis of the abdomen and/or flanks are at significant risk of vascular compromise to the abdominoplasty flap, given that these treatments have been shown to cause fibrosis of the superficial vascular network that is the main source of blood supply to the flap. Similarly, patients with a history of previous laser-assisted liposuction of the trunk have a compromised blood supply due to vascular fibrosis and coagulation of the treatment area. Extreme caution should be exercised when performing abdominoplasty in these patients, with or without liposuction.
Other general contraindications to circumferential liposuction of the trunk with abdominoplasty are the same as in any abdominoplasty procedure, which include significant medical conditions and future pregnancy.
Liposuction with Abdominoplasty
Traditional abdominoplasty has been well described by many investigators, including Matarasso, Lockwood, and others. Since the inception of liposuction in the late 1970s, surgeons have described various ways to combine abdominoplasty with liposuction to improve results. The concern of a higher rate of complications combining liposuction with abdominoplasty has prevented the widespread practice of this approach. Investigators reported a higher incidence of flap necrosis and seroma, among other complications, when liposuction is combined with abdominoplasty. Matarasso developed guidelines for the safe practice of liposuction with abdominoplasty based on the anatomic distribution of vascular supply to the trunk.
Why SAFE Lipo is Safe in Abdominoplasty
The SAFE Lipo technique allows for safe, consistent liposuction that does not damage flap blood supply, and can be easily taught to and is reproducible by other surgeons. This technique generates tremendous skin retraction while minimizing the risk of uneven scar adhesions and resultant irregular skin contour.
- 1.
Anatomic considerations: Blood supply of the abdominoplasty flap is from secondary sources, from superficial to deep subcostal and intercostal perforators that have already supplied the superolateral trunk and have passed through watershed zones to the flap, which now provide the blood supply to the flap, which is normally supplied by rectus abdominis perforator vessels. The sub-Scarpa’s fat of the flap is the last tissue to be supplied by these sources—acting parasitically on the blood supply. The excision of the sub-Scarpa’s fat of the undermined area decreases the oxygen demand of the flap, basically “unloading” the flap.
- 2.
The fat separation used in the SAFE Lipo technique is performed without suction, which prevents suction avulsion injury to blood vessels by the cannula. Blood vessels then remain intact while aspirating free, separated fat with small-diameter cannulas.
- 3.
Liposuction of the posterior trunk does not affect the blood supply of the abdominoplasty flap.
Fig. 1 shows anatomic zones by treatment.
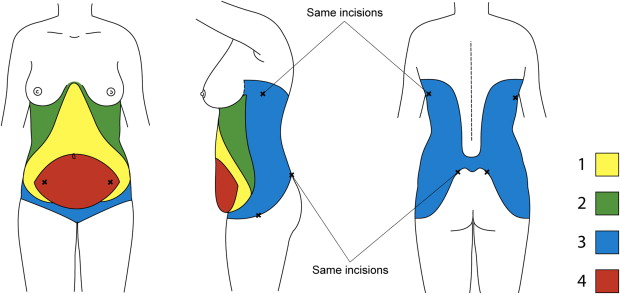
Anatomic Zones by Treatment
- 1.
Continuously undermined area of the final abdominoplasty flap—extending in a triangular fashion inferiorly from the xiphoid, extending infero-laterally to preserve the first 2 or 3 lateral perforators, extending further infero-laterally into the inferior portion of the flap.
- 2.
Discontinuously undermined area of thoracoabdominal area lateral to the flap—extending superiorly over the anterior aspect of the ribcage to the inframammary fold, laterally to the anterior axillary line, and inferiorly to beyond the lateral edge of the abdominoplasty incision.
- 3.
Remaining circumferential trunk—anteriorly to include the mons pubis, extending around the trunk to the back, limited superiorly by the inferior aspect of the axilla and the lower edge of the scapula, limited inferiorly by the lowermost aspect of the hip mound and sacrum.
- 4.
Abdominal pannus—to be excised.
Abdominoplasty Markings
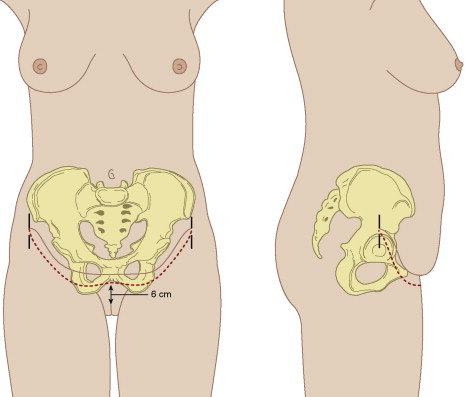
With the patient in the standing position, the anterior midline is marked from the xiphoid down to the anterior labial commissure. Using the top edge of the pubis as an underlying reference, the amount of lower abdominal skin ptosis is assessed, with the goal of producing a final scar location centrally to be at the top edge of the pubis. The lower abdominoplasty markings are made with the central point roughly 6 cm superior to the anterior labial commissure on full upward lifting of the skin (range of 4–7 cm), with a goal of elevating the ptotic mons pubis skin while allowing for full pannus excision ( Fig. 2 ). Usually the pannus includes all of the skin to above the umbilicus. If all of this skin cannot be excised to allow for closure, a small vertical closure results. If a vertical closure is unavoidable, the lower markings are placed as low as possible to allow the final scar to lie over the top edge of the pubis. Continuing laterally from the mons pubis, the markings are made with strong superomedial traction on the skin, using the desired location of the scar as a reference point. The desired location is directly over the top edge of the pubis centrally and 2 to 3 cm superior to the groin creases laterally, with the lateral aspect of the markings turning upward for the final 3 cm, stopping where no skin overhangs with light downward traction on the anterior abdominal skin. The upturned ends (2–3 cm) of the markings prevent downturned ends of the final scar location, allowing the final scar to run parallel to skin tension lines, in line with swimwear bottoms and without a conspicuous upturn or downturn of the ends of the scar. At the lateral extent of the markings, a reference mark drawn straight inferiorly is made to maintain orientation of the skin on closure. The strong medial advancement of the abdominoplasty flap can obscure the ends of the incision and these reference marks help maintain proper orientation. The lower abdominoplasty incision markings are not adjusted intraoperatively. Markings for the planned upper incision line gently arc to above the umbilicus or higher, depending on skin laxity with skin pinch, with the patient standing, bent forward with relaxed abdominal muscles. The markings for the upper incision line are only guides and are checked and verified intraoperatively, with the patient in the flexed position at the time of closure, with full downward tension on the abdominoplasty flap, just before excision of the pannus. The costal margins and xiphoid are marked as general reference points.
Liposuction Markings
Excluding the pannus to be excised, areas of excess fat are marked throughout the anterior abdomen with concentric circles, keeping in mind that the sub-Scarpa’s fat of zone 1 would be directly excised. The most prominent areas of excess in the flanks are marked, with concentric circles leading out from prominent areas. The midline of the back is marked. Areas of excess fat are identified by skin pinch, with the most prominent areas of the hips and any back rolls marked. Frequently there is midline lower back and sacral fat excess, which is also marked. The back marks are matched with the flank and abdominal markings, usually extending up to the inframammary folds and lower axillary areas in many patients.
Operative technique
Part I: Liposuction of the Circumferential Trunk with SAFE Technique
Before the induction of anesthesia, a thromboembolic disorder hose is placed and knee-high sequential compression devices (SCDs) (Compression Therapy Concepts, Eatontown, NJ, USA) are started. SCDs are sent home with the patient to be used for 48 hours or until the patient is completely ambulatory. The bladder is catheterized and preoperative antibiotics are given. The patient is maintained in a warmed room (77°C) until the warmed betadine prep and draping are completed. Warmed intravenous fluids and wetting solution are used, with the patient on a warmed bed (Cincinnati Sub-Zero Products, Inc, Cincinnati, OH, USA) throughout the procedure ( Fig. 3 ).
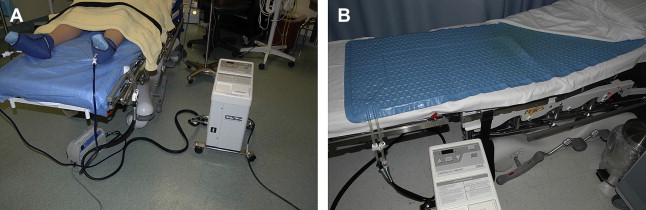
An esophageal temperature probe is used to maintain core temperature at 36°C or more. A single, whole-body prep is used for the procedure. A warmed betadine prep from the neck down to the knees is performed, turning the patient to each lateral decubitus position and placing sterile drapes beneath the patient as the prep progresses. Sterile stockinettes are placed over the lower extremities while another sterile drape is placed below the buttocks and lower extremities. The connectors for the SCDs are retrieved from the bottom of the stockinettes, and a second set of stockinettes is then rolled down to cover the SCD hoses. In this fashion, the sterile field is maintained from the upper chest down to the end of the operating table ( Fig. 4 ).
Related posts:
 Anatomic Considerations in Abdominoplasty
Anatomic Considerations in Abdominoplasty
 Editorial Comment on “Traditional Abdominoplasty”
Editorial Comment on “Lipoabdominoplasty: The Saldanha Technique”
Editorial Comment on “ SAFECircumferential Liposuction with Abdominoplasty”
Editorial Comment on “Concepts on Correction of the Musculoaponeurotic Layer in Abdominoplasty”
Revision Abdominoplasty and Proper Umbilical Positioning
Editorial Comment on “Traditional Abdominoplasty”
Editorial Comment on “Lipoabdominoplasty: The Saldanha Technique”
Editorial Comment on “ SAFECircumferential Liposuction with Abdominoplasty”
Editorial Comment on “Concepts on Correction of the Musculoaponeurotic Layer in Abdominoplasty”
Revision Abdominoplasty and Proper Umbilical Positioning
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


