Over the last decade in the minds of many plastic surgeons, the term “lipoabdominoplasty” has increasingly become synonymous with Dr Osvaldo Saldanha’s technique. I have had the pleasure of writing a discussion of an article in Plastic and Reconstructive Surgery about his technique, and I refer the reader to it for my in-depth analysis. On reading “Lipoabdominoplasty: The Saldanha technique” for this issue of Clinics in Plastic Surgery , I note that, as I have observed over the years, Dr Saldanha has further refined his technique and has made it easier to understand. I personally have used his technique, with a few modifications to suit my needs, and have found it to be an excellent addition to my armamentarium, especially in the patient who has a thick panniculus on presentation.
I would like to take this opportunity to make a few observations about Dr Saldanha’s technique. First, although it is an excellent idea to obtain an ultrasonogram of the abdomen in all patients who are to undergo an abdominoplasty, it is rather difficult to justify the cost to patients who are paying cash. Thus, at least in the United States, I believe that most surgeons can use ultrasonography only in a patient in whom they suspect a hernia.
Second, removing a horizontal ellipse of skin from the superior aspect of the mons pubis at closure (see Fig. 19 in “Lipoabdominoplasty: The Saldanha technique”) can be problematic in inexperienced hands. Although the purpose of excising this ellipse is to attain an aesthetic distance of 6 cm from the final scar to the vulvar commissure, the entire scar can potentially end up too high. In my experience, if there is a concern that the scar will migrate superiorly, then one should tack down Scarpa fascia of the mons pubis to the underlying rectus fascia at the desired level, which will help guarantee scar position. If that option is used, it is important to make sure that the abdominal flap will reach the tacked-down mons.
My third and final comment about Dr Saldanha’s article is the consistency of his preoperative marking measurements, “…initial markings always measured 28 cm in length—12 cm horizontally and 8 cm obliquely on each side.” In my practice, so many body types are present that I would find it difficult to use those measurements on all patients, especially those who present with high body mass indexes, very tall patients who are robustly built, and many massive weight loss patients. I suspect that Dr Saldanha has a more homogenous population than I do.
Related posts:
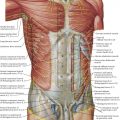 Anatomic Considerations in Abdominoplasty
Anatomic Considerations in Abdominoplasty
 Editorial Comment on “Traditional Abdominoplasty”
Editorial Comment on “ SAFECircumferential Liposuction with Abdominoplasty”
Editorial Comment on “Traditional Abdominoplasty”
Editorial Comment on “ SAFECircumferential Liposuction with Abdominoplasty”
 SAFECircumferential Liposuction with Abdominoplasty
Editorial Comment on “Concepts on Correction of the Musculoaponeurotic Layer in Abdominoplasty”
Revision Abdominoplasty and Proper Umbilical Positioning
SAFECircumferential Liposuction with Abdominoplasty
Editorial Comment on “Concepts on Correction of the Musculoaponeurotic Layer in Abdominoplasty”
Revision Abdominoplasty and Proper Umbilical Positioning
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


