DETERIORATION DUE TO CELLULITE
Author
Peter T. Pugliese, MD,
7139 Bernville Road, Bernville, PA 19506
Michael Q. Pugliese,LE,
Circadia by Dr Pugliese 8371 Route 183 Bethel, PA,19507
ABSTRACT
Perhaps no single cosmetic problem receives as much bad publicity as the subject of cellulite. To a great measure, this negative publicity is due to the many so-called experts in the field of cellulite. Scientific journals are replete within accurate descriptions of this condition. Greater success in dealing with this issue is hampered by the lack of basic understanding of this disorderthat produces emotional discomfort for a high percentage of women regarding their perception of beauty.
One would think a disorder that affects females almost exclusively would provide a clue to its cause. We call it a disorder because it is not truly a disease and in the true sense of the word, it is a natural consequence of a physiological process.
This chapter describes a possible explanation for the etiology of cellulite as well as suggestions for ingredients that can be useful in topical cosmetic applications. As far as the commonly known name, “cellulite,” this is sufficient for our purposes since the more technical name, “gynoid lipodystrophy,” does not shed any light on understanding the disorder, from a cosmetic point of view.
There are several reviews on the theories and treatment of cellulite, and for a more in-depth discussion, we refer the reader to reference 1.1 Keep in mind that much that has been written about cellulite in the past ten years is not based on accurate facts and we must dig a bit deeper to gain an understanding of what the phenomenon is, what causes it, and how to deal with it from a cosmetic point of view.
The term “adipose tissue” has taken on an entirely new meaning in the last ten years. We know now that this is not just a storage tissue, or a protective cushion. Rather, such tissue is actually a highly dynamic metabolic organ that has multiple functions. In this chapter we limit our discussion to cellulite and the adipose tissue. The reader, however, is referred to an interesting article on subcutaneous adipose tissue (2).
4.2.6.1 A Possible Etiology for Cellulite
4.2.6.3 The Matrix Metalloproteinases
4.2.6.4 The Menstrual Cycle, MMPs, and Ovulation
4.2.6.5 The MMPs and the Menstrual Cycle
4.2.6.6 The key step relating menses to the genesis of cellulite
4.2.6.7 Topical Therapy for Reversing the Appearance of Cellulite
a. Chysin—an aromatase inhibitor
4.2.6.8 Agents That Block MMPs
4.2.6.9 Mobilizing Adipose Tissue
4.2.6.10 Blocking Phosphodiesterase
4.2.6.11 Shuttling Fat into Mitochondria
4.2.6.1 A POSSIBLE ETIOLOGY FOR CELLULITE
First, we need to look at the anatomy of cellulite. True cellulite occurs only on the buttocks and thighs, to a distance about four inches above the knees. Obviously there will be some variations between individuals, but for the most part cellulite does not occur on the abdomen or the arms or the breasts. Why? The adipose tissue inthe buttocks and thighs is reserved for nutritional purposes in pregnancy during lean times. The adipose tissue in the upper thighs and buttocks contains twice as many alpha-2 receptors as it does beta receptors. The alpha-2 receptor inhibits lipolytic, or fat-burning, action so that this fatty tissue is not easily mobilized.2 This is why dieting and exercise are not very effective in the treatment of cellulite.
The second important area we must look at is the anatomical structure of the fat. The fatty tissue of men and women is structured in a series of connective tissue bands known as trabeculae. These tough collagen bands keep the fat in a somewhat ordered array and essentially two layers. See Figure 1 and Figure 1a below.
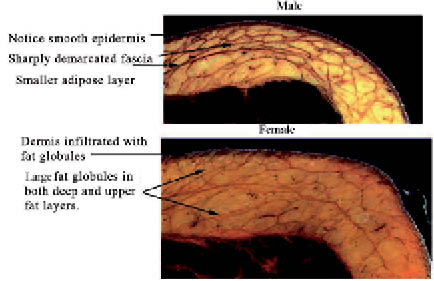
Figure 1. Human Anatomy of Thigh Skin: Male vs. Female
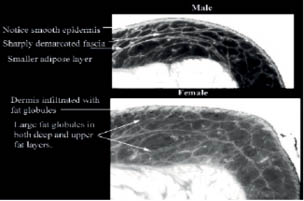
Figure 1a. Male vs. Female Adipose Tissue. Inverted Contrast.
There is a deep layer of fat that rests immediately upon the muscles. This in turn is separated by a superficial layer of fat immediately under the dermal layer of the skin,which is a thin fascia, and is called the superficial fascia.
Within the literature there are several errors that identify four to five layers of fat, along with a second major error that identifies male fatty distribution as being in a crisscross of compartment-like containers. This error has spread continuously throughout the cellulite literature, for it is quoted in just about every article one reads. No one to the author’s knowledge has ever duplicated the findings of this prior work by Nuremberger and Muller!i These investigators used two-dimensional histological preparations of skin. It is quite difficult to visualize a three- dimensional structure with this type of preparation. They also did not have the advantage of three-dimensional ultrasound studies.
Current studies employing 3-D ultrasound do not show evidence of crisscross collagen structure, or differences between male and female structure, other than the quantity and thickness of the collagen trabeculations (see Figure 2).The only distinguishing characteristicbetween male and female subcutaneous fat is the following:female fat is thicker, as measured from the bottom of the dermis to the muscle layer then in the male. The fat globules are generally larger than in the male adipose tissue. One can see this in Figure 1. Notice the size of the lobules and the thicknessof the fatty layers.
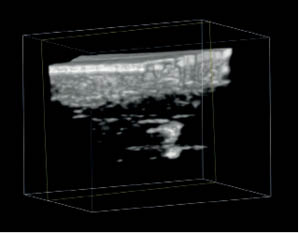
Figure 2. A 3-D Ultrasound of a 5-cm square section of cellulite thigh skin from a 28-year-old female. Taken with 7.5 mHz transducer.The black area represents the adipose tissue. Fat does not reflect ultrasound.
In cellulite, the primary structural abnormality lies in the disruption of the described collagen connective tissue bands. The collagen is known as Type I collagen, a tough ubiquitous structural component. In cellulite these bands are dissolved, either completely or partially, resulting in a disorganized and chaotic adipose tissue layers. This can be seen again in Figure 1 but can be more readily demonstrated by a 3-D ultrasound as seen in Figure 2.
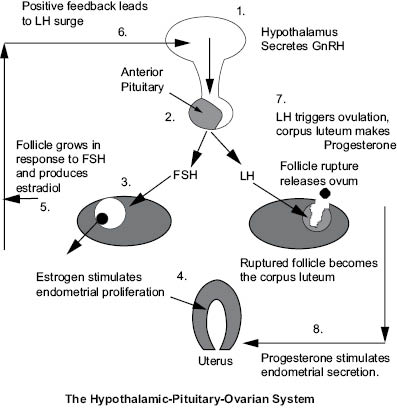
The immediate question arises:What could possibly cause such destruction in an otherwise well- organized tissue? The answer is very surprising. It took one author, P.T. Pugliese, M.D.,tenyears to appreciate the fact that cellulite is not a fat disorder; rather,it is a consequence of another innocuous physiological process, collagenase destruction of endometrium. Dr. Pugliese searched for a source of collagenase in the body that would have the power to dissolve type I collagen and which appears almost immediately after puberty.3 The menstrual cycle appeared to be the most likely candidate. To appreciate the role of the menstrual cycle and the associated hormones and enzymes in the genesis of cellulite we must review the physiology of the menstrual cycle.
Briefly, the menstrual cycle produces a succulent hospitable environment for a pregnancy. In the absence of pregnancy, endometrium of the uterus (inner lining) must be discarded and renewed on a monthly basis. The renewable environment is known as the endometrium, and it greatly enlarges during the early phase of the menstrual cycle under the influence of estrogen. The major structural components are a collagen type I matrix and an adequate supply of small blood vessels. This is shown in Figure 3. While the hormone relationship is fairly well understood, the role of the destructive enzymes and associated cytokines is less well understood. The following explanation represents our current understanding of the biological compounds involved in the menstrual cycle.
4.2.6.3 THE MATRIX METALLOPROTEINASES
In the absence of a pregnancy, estrogen and progesterone fall to very low levels. This initiates a process that removes the endometrium by a collagenolytic process called shedding. Specific enzymes known as matrix metalloproteinases cleave the collagen fibers and break them down into peptides and amino acid, which are recycled in the metabolic pool. These enzymes originate from fibroblasts and perhaps other cells of the endometrium stromal cells in particular. These special enzymes are called matrix metalloproteinases, or MMPs.
Related posts:
 – THE CELLULAR WATER PRINCIPLE
– THE CELLULAR WATER PRINCIPLE
 – BIOACTIVES GREEN AND SUSTAINABLE INGREDIENTS FROM BIOTRANSFORMATION AND BIOFERMENTATION
– BIOACTIVES GREEN AND SUSTAINABLE INGREDIENTS FROM BIOTRANSFORMATION AND BIOFERMENTATION
 – PEPTIDES FOR ANTI-AGING SKIN CARE
– PEPTIDES FOR ANTI-AGING SKIN CARE
 – CHRONOBIOLOGY OF THE SKIN SKIN CIRCADIAN RHYTHM AND CLOCK GENES: A NEW APPROACH TO SLOWING DOWN THE AGING PROCESS
– CHRONOBIOLOGY OF THE SKIN SKIN CIRCADIAN RHYTHM AND CLOCK GENES: A NEW APPROACH TO SLOWING DOWN THE AGING PROCESS
 – SKIN WHITENER INGREDIENTS
– SKIN WHITENER INGREDIENTS
 – AMINO ACIDS
– AMINO ACIDS
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


