Tissue Expander With Acellular Dermal Matrix
Gabriel M. Kind
DEFINITION
Two-stage tissue expander-to-implant reconstruction with prosthetic implants is the most common type of breast reconstruction in the United States.1,2
The use of acellular dermal matrix (ADM), originally described for direct-to-implant reconstruction,3,4 has become increasingly common in two-stage procedures as well.5,6,7
The potential benefits of this technique include more precise recreation of the inframammary fold (IMF), control of the pectoralis major muscle, reduced risk of implant palpability, reduction in capsular contracture rates, and a larger initial expander volume (and consequently fewer office visits for tissue expansion), with less dissection of the chest wall musculature when compared to total muscle coverage of the tissue expander (TE).
All of these potential benefits would presumably improve aesthetic results and, at least for the latter benefit, result in less morbidity.
Recently, there have been reports describing the placement of implants wrapped with dermal allograft in the prepectoral position.
This technique has the potential to decrease the incidence of some of the muscle-related complications associated with subpectoral placement, namely, pain associated with manipulation of the muscle at the initial surgery, discomfort associated with pectoralis major flexion postoperatively, and the animation deformity seen in some patients with flexion of the pectoralis major muscle.8
ANATOMY
The pectoralis major muscle has sternocostal, costal, and abdominal origins and inserts on to the proximal humerus. It is a type V muscle, with a dominant arterial pedicle from the thoracoacromial trunk and multiple secondary arterial sources from parasternal perforators.
PATHOGENESIS
Breast cancer occurs in approximately 12% of women in the United States. It is estimated that nearly 250 000 new cases of invasive breast cancer will be diagnosed in 2016, along with 61 000 cases of in situ disease.
Although there are significant regional differences, mastectomy is performed in approximately 35% of those newly diagnosed, and approximately 35% of those women undergo breast reconstruction.
The rate of breast reconstruction has risen steadily, from 11.6% in 1998 to 36.4% in 2011.9
In 2014, of the 102 215 breast reconstructions performed in the United States, 74 694 (73%) used a TE and implant.2
PATIENT HISTORY AND PHYSICAL FINDINGS
The use of dermal allograft for soft tissue support at the time of mastectomy is an intraoperative decision based on several factors, including the thickness of the mastectomy skin flaps, the anatomy of the pectoralis major muscle, and the desired initial volume of the TE.
If ADM is not used, either a total submuscular pocket is created or partial muscle coverage of the expander is accepted.
IMAGING
Not indicated or necessary
SURGICAL MANAGEMENT
Preoperative Planning
The footprint of the breast is measured. The height and width of the breast are used to determine which TE to order. Usually two or three differently sized expanders are ordered for each case.
If mastectomy has already been performed, the pectoralis major muscle function is assessed. Rarely, a paralytic or atretic muscle is identified preoperatively. In such cases, a larger piece of ADM may be necessary.
Positioning
The patient is placed supine with both arms abducted and secured on well-padded arm boards or tucked depending upon surgeon preference.
Approach
There are a number of different incisions used for mastectomy. TE insertion can be performed via any of the incisions used.
In nipple-sparing procedures, care should be taken to avoid handling of the nipple to decrease the chance of contamination. Adhesive plastic drapes can be placed for this purpose.
TECHNIQUES
▪ Subpectoral Tissue Expander Placement With Dermal Allograft
Markings
The footprint of the breast, including the IMF, is marked with the patient standing and again under anesthesia.
Once the mastectomy is completed, hemostasis is confirmed.
Creation of Subpectoral Pocket
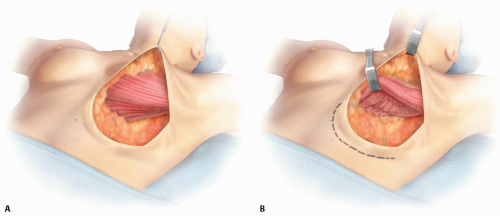
The pectoralis major muscle is elevated to create a subpectoral pocket across the footprint of the breast (TECH FIG 1). The sternocostal origin is released as necessary.
There is significant variability in the location of the origin of the pectoralis major muscle.
Muscle attachments are preserved wherever possible. This will reduce the size of the ADM required.
Preparation and Suturing of Dermal Allograft
A sheet of dermal allograft is prepared by irrigating it with normal saline followed by antibiotic solution. ADM is provided in various sizes.
Generally 4 to 8 cm × 14 to 18 cm sheets are used; more recently shaped pieces have become available.
Prefenestrated ADM is used, or fenestrations are cut into the ADM, to encourage revascularization.
The use of thick or thin ADM also depends upon the preference of the surgeon.
Care is taken to place the dermal (shiny) side of the ADM facing the undersurface of the mastectomy flaps.
The dermal allograft is sutured to the chest wall along the desired position of the IMF.
I prefer running absorbable barbed suture (2-0 PDO Quill) for this, although other suture types have been described, perhaps most commonly some type of an absorbable suture is used.
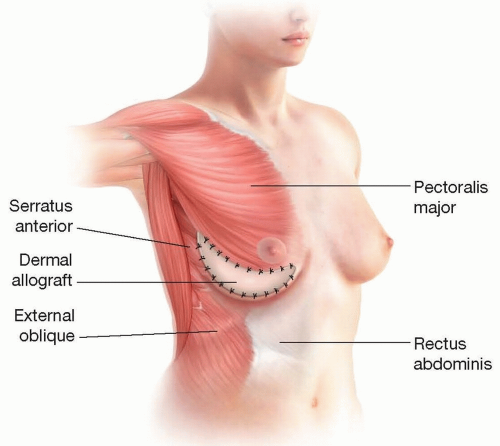
TECH FIG 1 • A,B. The pectoralis major muscle is elevated across the footprint of the breast.
TECH FIG 2 • The dermal allograft is secured to the IMF. The ADM is secured along the IMF to a point equal or superior to the vertical midpoint of the breast.
The lateral extent of the ADM-IMF suture line should be at least to a point equal to the vertical midpoint of the breast.
Patients with thin mastectomy flaps may benefit from continuing the ADM further superolaterally, but this may tether the pectoralis major and is generally not required (TECH FIG 2).
Preparation and Placement of Tissue Expander
A TE is selected based on the width of the breast footprint, the weight of the mastectomy specimen, and the patient’s desired size.
The TE is prepared by removing the air and inserting 50 to 100 mL of saline.
Some prefer methylene blue-tinted saline, whereas others prefer to fill the expander with air.
The TE is placed in the wound and secured in place using 2-0 PDS suture if suture tabs are utilized. For expanders without tabs, precise pocket formation will limit movement of the expander.
The ADM is trimmed to fit the defect in the inferolateral aspect of the subpectoral pocket.
The upper border of the ADM is sutured to the lower border of the pectoralis major muscle (TECH FIG 3).
Additional saline is injected into the TE.
In a total skin and nipple-sparing mastectomy, the expander is filled to approximately 50% of its capacity.
In non-nipple-sparing mastectomies, the final volume is determined by the limitation of the skin flaps.
Closure
Closed suction drains are placed through stab incisions in the lateral chest wall.
For larger breasts and cases where axillary dissection is performed, two drains are used. For smaller breasts, one drain is used.Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree