■ Computed tomography (CT). A preoperative neck or chest CT is usually not necessary except in specific situations:
■ Malignancy—A neck CT may suggest local invasion of the thyroid into surrounding structures such as the carotid artery, internal jugular vein, or trachea which could potentially modify the operative approach. A CT scan of the neck can also provide a detailed map of cervical lymphadenopathy. A chest CT can evaluate for metastatic disease.
■ Large goiters—A neck and chest CT scan can help determine the degree of tracheal obstruction or substernal extension of large goiters. Patients with clinical evidence of airway obstruction should have a CT to provide anatomic information to help manage a potentially difficult airway.
■ Laryngoscopy. Flexible laryngoscopy should be performed on all patients with hoarseness or a previous history of neck surgery. This provides a current assessment and baseline evaluation of bilateral vocal cords prior to surgery.
SURGICAL MANAGEMENT
■ Thyroid lobectomy is therapeutic for patients with a unilateral goiter or a solitary toxic nodule which is symptomatic.
■ Thyroid lobectomy is diagnostic and can potentially be therapeutic for patients with indeterminate thyroid nodules such as those categorized as “follicular lesions of undetermined significance,” “follicular neoplasms,” or “suspicious for malignancy.”
■ Although thyroid malignancy often warrants surgical intervention, thyroid lobectomy is typically not the standard of care. Total thyroidectomy is recommended for most thyroid malignancies greater than a centimeter in size. A thyroid lobectomy may sometimes be appropriate for very small (less than a centimeter) well-differentiated thyroid cancers in select patients.
■ In any thyroid lobectomy, the patient and surgeon should be prepared for the conversion to a total thyroidectomy if intraoperative findings dictate this need. If the patient was not counseled of this possibility, the surgeon should complete the lobectomy and defer definitive management until appropriate consent from the patient.
Preoperative Planning
■ Thyroid lobectomy is performed under a general anesthesia, but locoregional anesthetic with sedation may be adequate for lobectomy in select patients.
■ Routine use of preoperative antibiotics is not common as wound infections after thyroid lobectomy are rare.4
Positioning
■ The patient is placed in the supine position with the arms padded and tucked at the side (FIG 1). A roll can be placed under the shoulders to help extend the neck; however, extreme extension should be avoided as this can cause postoperative discomfort.
TECHNIQUES
SKIN INCISION AND FLAP CREATION
■ A low collar incision is placed symmetrically across the neck despite only removing a lobe. The incision is ideally located about two fingerbreadths above the sternal notch or 1 cm below the cricoid cartilage (FIG 2). This location provides good exposure to the entire thyroid gland and particularly the superior pole.
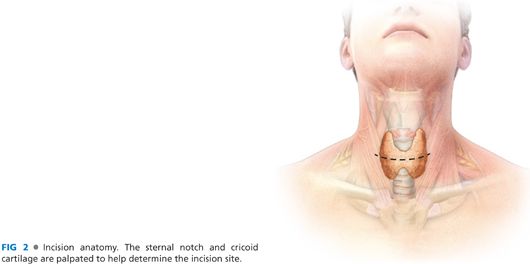
■ Placing the incision in a skin crease can provide excellent cosmetic results. If no skin crease is appropriate, Langer’s lines provide an adequate guide.
GLAND EXPOSURE
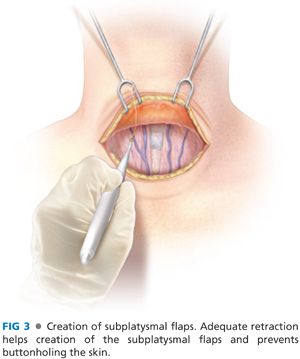
■ The incision is carried through the subcutaneous tissue and platysma. Subplatysmal flaps are created to enhance mobility from the incision (FIG 3). These flaps should extend to the thyroid cartilage superiorly and the suprasternal notch inferiorly. The assistant should retract the skin to help create the plane of dissection. The anterior jugular veins will remain down on the strap muscles if the correct plane is dissected.
■ The midline raphe between the strap muscles is opened and dissection extends down to the level of the isthmus (FIG 4).
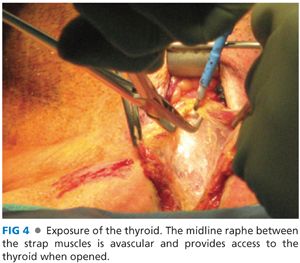
■ The sternohyoid and, subsequently, the sternothyroid muscles are dissected off the thyroid and reflected laterally.
■ The thyroid lobe is then retracted medially with a finger or hemostatic clamp. The space between the thyroid and the carotid sheath is opened bluntly until the prevertebral fascia is encountered (FIG 5
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


