Chapter 5
The Upper Limb
- Embryology
- Congenital deformities
- Hand trauma
- Hand infections
- Complex regional pain syndrome (CRPS)
- Nerve compression
- Traumatic brachial plexus injury
- Obstetric brachial plexus palsy
- Tendon transfers
- Dupuytren’s disease
- Tumours
- Arthritis
- Miscellaneous tendinopathy
- Further reading
Embryology
Developmental anatomy
- Upper limb bud appears in the flank of the embryo on day 26.
- Consists of a core of lateral plate mesoderm covered by ectoderm.
- This mesoderm will differentiate into bone, cartilage and tendon.
- Ectoderm thickens at the tip of the bud in the anteroposterior (AP) axis to form the apical ectodermal ridge (AER).
- In the embryo, the AP axis is analogous to the radio-ulnar axis.
- The limb bud is initially supplied by a capillary network.
- This coalesces into a main stem artery that drains into a marginal vein.
- Artery becomes the subclavian-axillary-brachial axis.
- Vein becomes the basilic-axillary-subclavian axis.
- The brachial artery branches into interosseous and median arteries.
- The median artery provides the main blood supply to the hand.
- It is usually replaced by ulnar and radial arteries around day 44.
- Regresses to provide the blood supply of the median nerve.
- By day 33 a paddle-shaped hand is present.
- Prechondrogenic condensations of mesenchyme appear where skeletal elements will form.
- Around day 36, nerve trunks enter the arm.
- Somitic mesoderm invades the limb and aggregates into dorsal and ventral masses.
- These differentiate into myoblasts that become muscle.
- By day 42, digital rays are present and the hand assumes a webbed appearance.
- During the 7th week, upper limbs rotate 90° laterally to bring the palm anteriorly.
- At the same time, the elbow begins to flex.
- During this period, ossification begins and digital separation occurs.
- This occurs by the apoptosis of tissue between finger rays.
- By the 8th week, the upper extremity resembles a miniature adult upper limb.
- Consists of a core of lateral plate mesoderm covered by ectoderm.
Mechanisms of development
- Our understanding comes largely from transplanting tissue within chick embryos.
- Discrete cell signalling pathways establish the three axes of limb development:
Proximodistal axis
- Controls how the limb differentiates into a shoulder proximally but fingers distally.
- The critical area is the AER.
- Resection of the AER results in a truncated limb.
- Earlier resection results in more proximal limb truncation.
- Grafting of the AER elongates limbs of chick embryos.
- Resection of the AER results in a truncated limb.
- AER produces fibroblast growth factors (FGFs), most importantly FGF 2, 4 and 8.
Anteroposterior axis
- Controls how an ulna and little finger develop on one side but a radius and thumb on the other.
- The critical area is the zone of polarising activity (ZPA).
- ZPA is a cluster of mesenchymal cells in the posterior limb bud margin.
- Grafting of ZPA cells to the anterior limb margin induces mirror image duplication.
- ZPA is a cluster of mesenchymal cells in the posterior limb bud margin.
- The ZPA produces Sonic hedgehog (Shh).
- Higher concentrations of Shh result in more posterior (ulnar) digits being formed.
- Cells of the AER and ZPA are interdependent:
- FGFs from the AER are required for Shh expression.
- Shh signal is required to maintain AER integrity.
- FGFs from the AER are required for Shh expression.
- This may explain why loss of elements often occurs in both AP and proximodistal axes.
Dorsoventral axis
- Controls how the limb differentiates into a dorsal and palmar surface.
- The critical area is non-AER ectoderm.
- Removing and replacing ectoderm from a chick limb bud, having reversed its dorsoventral polarity, will produce a reversal in the polarity of the underlying mesoderm.
- Wnt-7a is a protein encoded by the WNT7A gene.
- WNT7A is expressed specifically by dorsal limb ectoderm and determines dorsal limb identity, e.g. fingernails.
- Wnt-7a activates expression of LIM homeodomain factor Lmx1.
- WNT7A is expressed specifically by dorsal limb ectoderm and determines dorsal limb identity, e.g. fingernails.
- In contrast, ventral ectoderm expresses engrailed-1 (en-1), which inhibits Wnt-7a and restricts its actions to the dorsal ectoderm.
- Failure of these systems produces duplicated palms or circumferential fingernails.
Congenital deformities
Classification
- Swanson’s classification is widely accepted.
- The following account does not include the full hierarchy of the classification:
I. Failure of formation of parts (arrest of development)
A. Transverse arrest
- Shoulder, arm, elbow, forearm, wrist, carpal, metacarpal, phalanx.
B. Longitudinal arrest
- Radial ray
- Ulnar ray
- Central ray (cleft hand)
- Intersegmental (intercalated) type of longitudinal arrest.
II. Failure of differentiation (separation) of parts
A. Soft tissue involvement
- Arthrogryposis
- Cutaneous syndactyly
- Camptodactyly
- Thumb-in-palm deformity
B. Skeletal involvement
- Clinodactyly
- Osseous syndactyly
- Symphalangia
- Elbow, forearm and carpal synostosis.
C. Congenital tumorous conditions
III. Duplication
- Whole limb, humerus, radius, ulna
- Mirror hand
- Radial polydactyly (preaxial polydactyly)
- Central polydactyly
- Ulnar polydactyly (postaxial polydactyly).
IV. Overgrowth
- Whole limb
- Macrodactyly.
V. Undergrowth
- Whole limb, whole hand
- Brachymetacarpia
- Brachysyndactyly, with or without absence of pectoral muscle
- Brachydactyly.
- Brachymetacarpia
VI. Congenital constriction band syndrome
- Constriction band either with or without lymphoedema
- Acrosyndactyly
- Intrauterine amputation.
VII. Generalised skeletal abnormalities
- Chromosomal abnormalities
- Other generalised abnormalities.
- This classification is based on work published in the 1960s and 1970s.
- As understanding of the pathogenesis has progressed, the shortcomings of the classification have become evident.
- Differentiating between transverse arrest, brachysyndactyly and symbrachydactyly (previously termed atypical cleft hand) can be difficult:
- Some consider brachysyndactyly and symbrachydactyly to be the same entity, on a continuum with transverse arrest, rather than classified as undergrowth.
- Buck-Gramcko wrote in 1999: ‘The Congenital Committee of the IFSSH has recognized the problem of symbrachydactyly classification since 1995 but has not come to any conclusions and recommendations’.
- Swanson himself noted: ‘Brachysyndactyly could be placed in either Category I or II because of some of its features… Its most obvious failure clinically, however, is hypoplasia or undergrowth, and for that reason it is placed in Category V’.
- Some consider brachysyndactyly and symbrachydactyly to be the same entity, on a continuum with transverse arrest, rather than classified as undergrowth.
Failure of formation
Transverse arrest
- Can occur at any level.
- Most common at the junction of proximal and middle thirds of the forearm.
- Treatment is usually non-surgical with a prosthesis from 6 months.
- Children with unilateral deformities tend to discard the prosthesis.
- When there are metacarpal remnants, these may be amenable to:
- Distraction lengthening
- Free phalangeal or toe transfer.
- Distraction lengthening
Longitudinal arrest
Radial deficiency
- A spectrum of abnormalities affecting the radial side of the forearm.
- Radius, radial carpus, thumb, tendons, ligaments, muscles, nerves and blood vessels can all be involved.
- Most common type of longitudinal failure of formation, affecting one in 55,000 live births.
- Usually manifests as hypoplastic or absent radius with radial deviation of the hand—formerly known as ‘radial club hand’.
Associated abnormalities
- Up to 40% of unilateral and 77% of bilateral cases are syndromal.
- All require assessment by a paediatrician and geneticist.
- Associated conditions include:
- Holt–Oram syndrome
- Cardiac septal defects and various upper limb malformations.
- Autosomal dominant inheritance.
- Cardiac septal defects and various upper limb malformations.
- VACTERL association
- Vertebral anomalies, Anal atresia, Cardiac defects, Tracheal anomalies (including tracheo-oesophageal fistula), Esophageal atresia, Renal and radial abnormalities, other Limb abnormalities.
- TAR syndrome
- Thrombocytopaenia-Absent Radius; autosomal recessive inheritance.
- The thumb is usually present in TAR.
- Thrombocytopaenia-Absent Radius; autosomal recessive inheritance.
- Fanconi’s anaemia
- Rare autosomal recessive cause of bone marrow failure.
- Radial deficiency affects 40%; aplastic anaemia develops around 6 years.
- Fatal without bone marrow transplantation.
- Rare autosomal recessive cause of bone marrow failure.
- Holt–Oram syndrome
Clinical features
- Short forearm, bowed on the radial side.
- Complete or partial absence of the radius, which may be replaced by a fibrous anlage.
- [In German, Anlage (pronounced ann-lager), means ‘foundation’ or ‘plan’]
- Radially deviated hand with reduced passive wrist motion.
- Radial skin deficiency with relative excess on the ulnar side.
- Hypoplastic or absent thumb.
- Flexion contracture and stiffness of the radial digits.
- Elbow stiffness, which may be due to bony fusion (synostosis).
- Proximal muscles of the arm and shoulder can also be affected.
- Bilateral and unilateral involvement are equally common.
- Involvement of the contralateral limb may be subtle and asymmetric.
Classification
- Classified into four types by Bayne and Klug:
- Type I: Short distal radius
- Type II: Hypoplastic radius
- Type III: Partial absence of the radius
- Type IV: Total absence of the radius.
- Type I: Short distal radius
Treatment
- Based on age, severity and degree of functional deficit.
Manipulation
- Physiotherapy to elbow and wrist prevents progressive stiffness and maintains range of motion.
- Parents should do this at least twice a day.
- Mildest deformities can be treated with physiotherapy alone.
- Splintage is difficult to apply and adds little benefit.
- External fixators are widely used to distract radial soft tissues prior to surgery.
Surgery
- Performed around 12 months, but this varies.
- The following abnormalities may be found:
- Variable deficiencies of the radial forearm structures.
- Aberrant radial wrist extensors and extrinsic thumb muscles.
- Absence of the radial artery.
- Absence of the radial nerve below the elbow.
- Median nerve is always present—often the most radial structure of the wrist.
- Variable deficiencies of the radial forearm structures.
- Centralisation
- Carpus is repositioned over the ulna and stabilised with a pin through the third metacarpal and carpus into the ulna.
- Usually requires extensive soft tissue release.
- Radial wrist extensors are transposed onto extensor carpi ulnaris (ECU) to counter the radial deforming force.
- Some recommend transposing redundant skin from the ulnar wrist to release the radial contracture.
- Carpus is repositioned over the ulna and stabilised with a pin through the third metacarpal and carpus into the ulna.
- Radialisation
- Scaphoid is placed over the ulna and secured with a pin through the second metacarpal.
- Transfer of flexor carpi radialis (FCR) and flexor carpi ulnaris (FCU) to the ulnar carpus or fifth metacarpal decreases the radial deforming force.
- Scaphoid is placed over the ulna and secured with a pin through the second metacarpal.
- Microvascular joint transfer
- Centralisation and radialisation are associated with high recurrence rates.
- They also have the potential to injure the distal ulnar physis, causing growth arrest.
- Vilkki described vascularised transfer of the second MTPJ to avoid these problems.
- It is technically demanding and not widely practised.
- Centralisation and radialisation are associated with high recurrence rates.
- Pollicisation of the index finger
- Indicated for cases with a severe hypoplastic thumb.
- Aims to reproduce thumb function by shortening and rotating the index finger.
- A radial palmar incision is made, creating skin flaps at the base of the index finger.
- Allows subsequent creation of a first webspace.
- Ulnar digital nerve is mobilised by interfascicular dissection of the common digital nerve to the index-middle finger web.
- Radial digital artery to the middle finger is ligated and divided.
- Interossei are elevated from the index finger metacarpal.
- Index metacarpal is removed, except for its head, which forms the new trapezium.
- The epiphysis is resected to prevent subsequent growth.
- Metacarpal head is rotated 160°—this will subsequently relax to 120°, ideal for opposition.
- Secured with K wires in 40° of palmar abduction with metacarpophalangeal joint (MCPJ) hyperextended.
- The length of metacarpal removed is measured and a similar length of flexor and extensor tendon is excised.
- Some do not remove tendon because they are said to shorten over time.
- Rebalancing the intrinsics is essential:
- First dorsal interosseous is sutured to the radial lateral band to become abductor pollicis brevis (APB).
- First palmar interosseous is sutured to the ulnar lateral band to become adductor pollicis.
- Extensor indicis proprius (EIP) acts as extensor pollicis longus (EPL).
- Extensor digitorum communis (EDC) to the index finger acts as the abductor pollicis longus (APL).
- Many children require opponensplasty between 5 and 8 years.
- A radial palmar incision is made, creating skin flaps at the base of the index finger.
- Indicated for cases with a severe hypoplastic thumb.
Ulnar deficiency
- One-tenth as common as radial deficiency.
- Spectrum of abnormalities, from hypoplasia of ulnar digits to absence of ulna.
- Hand and carpus are always affected: missing digits, syndactyly, thumb abnormalities.
- It differs from radial deficiency:
- The wrist is stable but elbow unstable.
- Associated more with musculoskeletal abnormalities than cardiovascular.
- Total absence is most common for the radius; partial absence is most common for the ulna.
- Less likely to occur as part of a syndrome.
- The wrist is stable but elbow unstable.
Classification
- Classified by Bayne into four types:
- Type I: hypoplasia of the ulna (both proximal and distal epiphyses present)
- Type II: partial aplasia of the ulna (absence of the distal or middle third)
- Type III: total aplasia of the ulna
- Type IV: radiohumeral synostosis.
- Type I: hypoplasia of the ulna (both proximal and distal epiphyses present)
Treatment
- Depends on the nature and severity of the deformity; there is no consensus view.
- Release of the fibrous anlage with realignment of the carpus and forearm.
- The anlage, present in types II and IV, is claimed to increase ulnar deviation of the hand and ulnar bowing of the radius as the child grows.
- Hand function is improved as required by:
- Separating any syndactyly
- Deepening the first webspace
- Thumb reconstruction: opponensplasty, rotation osteotomy or pollicisation.
- Separating any syndactyly
- Rotation osteotomy of the humerus improves hand position for some cases of radiohumeral synostosis.
Central deficiency
- Also known as cleft hand.
- Historically, cleft hand was divided into typical and atypical types.
Typical cleft hand
- V-shaped cleft in the centre of the hand; one or more digits may be absent.
- Often bilateral; frequently involves both the hands and feet.
- Family history is common—inheritance is autosomal dominant.
- May form part of a syndrome, e.g. split-hand/split-foot, EEC (ectrodactyly, ectodermal dysplasia, facial clefts).
- First webspace often narrowed.
- ‘Transverse metacarpals’ can further widen the cleft over time.
- Phalanges may have longitudinally bracketed epiphyses or duplications.
Classification of typical cleft hand
- The Manske and Halikis classification focuses on the first webspace:
- Type I: normal web
- Type IIA: mildly narrowed web
- Type IIB: severely narrowed web
- Type III: syndactylised web (first webspace is obliterated)
- Type IV: merged web (index ray suppressed; first webspace merged with the cleft)
- Type V: absent web (thumb elements suppressed; first webspace not present).
- Type I: normal web
Treatment of typical cleft hand
- Patients usually have good hand function.
- Labelled ‘a functional triumph, but a social disaster’.
- Early surgery may be required to prevent progressive deformity:
- To separate syndactyly between unequal digits, especially thumb-index.
- To remove transverse bones that would worsen the cleft with growth.
- To separate syndactyly between unequal digits, especially thumb-index.
- Other surgery can be postponed until between 1 and 2 years:
- Release or reconstruction of the first webspace.
- Closure of the cleft.
- Snow-Littler technique: palmar-based flap from the cleft is transposed to the first web.
- Miura and Komada method: simpler—palmar and dorsal flaps are redraped.
- 2nd metacarpal is transferred to the 3rd metacarpal base and secured with K wires.
- Transposing the 2nd metacarpal at the level of its neck may preserve the adductor pollicis origin from the 3rd metacarpal.
- Deep transverse metacarpal ligament is reconstructed using adjacent A1 pulleys, unfolded towards one another.
- Snow-Littler technique: palmar-based flap from the cleft is transposed to the first web.
- Creation of a thumb for cases where it is absent.
- Pollicisation or, if no radial ray available, free toe transfer.
- Addressing the foot deformity
- Only indicated when there are difficulties fitting footwear.
- The fibular ray is the most important for weight bearing and gait.
- The tibial toe can usually be transferred to the hand if required.
- Only indicated when there are difficulties fitting footwear.
- Release or reconstruction of the first webspace.
Atypical cleft hand
- Now known as symbrachydactyly.
- Characterised by short vestigial digits, like small nubbins.
- Often have vestigial nails.
- May occur with Poland’s syndrome.
- Symbrachydactyly, in contrast to central ray deficiency:
- Is usually unilateral
- Seldom involves the feet
- Is not usually associated with a family history.
- Is usually unilateral
- Its place within Swanson’s classification is controversial.
- Probably not a longitudinal central ray deficiency.
Classification of symbrachydactyly
- Blauth and Gekeler classify symbrachydactyly into four types:
- Short finger type—a thumb and four short stiff digits
- Oligodactylic type—central aplasia—the classic ‘atypical cleft hand’
- Monodactylic type—a thumb and four nubbins
- Peromelic type—complete absence of fingers and thumb.
- Short finger type—a thumb and four short stiff digits
Treatment of symbrachydactyly
- Short finger type usually have excellent function.
- Some may require syndactyly release or free phalangeal bone transfer.
- Oligodactylic type achieve pincer grip with thumb and little finger.
- Metacarpal rotation osteotomy can improve the position of these digits.
- Some oligodactylic and monodactylic types may be suitable for toe-to-hand transfers if metacarpals and extrinsic tendons are present.
- Peromelic type is difficult to reconstruct due to lack of proximal structures.
Intersegmental deficiency
- ‘Phocomelia’ is the historical term for intercalated deficiency of the upper limb.
- Phocomelia derives from the Greek, meaning ‘seal limb’, i.e. a flipper.
- The hand is always present.
- Prevalent in the 1960s due to the use of thalidomide for hyperemesis gravidarum.
- Worldwide, thalidomide is still used as an anti-angiogenic drug to treat leprosy and myeloma.
- Frantz and O’Rahilly classify phocomelia into three types:
- Type I: complete—the hand is directly attached to the trunk
- Type II: proximal—the forearm and hand are attached to the trunk
- Type III: distal—the hand is attached to the humerus at the elbow.
- Type I: complete—the hand is directly attached to the trunk
- A prosthesis may be required if the hand cannot reach the mouth.
- Surgery, usually to stabilise the limb, is rarely indicated.
Failure of differentiation
Soft tissue failures of differentiation
Syndactyly
- Derived from the Greek, ‘syn’—‘together’ and ‘dactylos’—‘digit’.
- May result from failure of apoptosis in interdigital tissue.
- Occurs once every 2000 live births.
- One of the two most common upper limb malformations, the other being polydactyly.
- 20% have a family history (autosomal dominant); 50% are bilateral.
- Twice as common in males.
- Most common in Caucasian races.
- May be associated with other deformities such as Apert’s and Poland’s.
Classification
- Complete—digits fused to the level of the tips.
- Incomplete—fusion does not extend to the tips.
- Simple—only soft tissue connections between the digits.
- Complex—soft tissue and bony connections between the digits.
- Complex complicated—associated accessory digits or phalanges within the syndactyly.
- Acrosyndactyly—characterised by fused distal parts of the fingers.
- Small spaces (fenestrations) are always present between the digits proximally.
- Pathogenesis of acrosyndactyly is different from other forms of syndactyly:
- Distal parts of the digits are thought to re-fuse due to constriction ring syndrome.
- Small spaces (fenestrations) are always present between the digits proximally.
Clinical features
- Middle-ring finger web is most commonly affected—58% of cases.
- 27% ring-little finger web.
- 14% middle-index web.
- 1% thumb-index web.
- 27% ring-little finger web.
- Nail fusion (synonychia) with loss of the paronychial fold suggests synostosis of the distal phalanges.
- Associated limb, chest wall and foot abnormalities.
- Radiographs may show synostosis, synpolydactyly or other anomalies.
- More complex syndactyly is associated with tendon, nerve and vessel anomalies.
- Variable vascular anatomy and distal bifurcation of common digital vessels can lead to vascular compromise following separation.
Indications for surgical correction
- Not usually performed before 1 year of age.
- Aim to have separation completed by school age.
- Indications for earlier surgery, as soon as the child is deemed fit, include:
- Syndactyly of thumb-index or little-ring fingers.
- Released early because length discrepancy can cause deformity with growth.
- Syndactyly of thumb-index or little-ring fingers.
Principles of surgical correction
- Aim to separate the digits, provide a lined commissure, create minimal scarring.
- The normal webspace slopes 45° dorsal to palmar and runs from the metacarpal heads to the midpoint of the proximal phalanx.
- Most techniques share the following principles:
- Release only one side of a digit at a time to avoid jeopardising finger vascularity.
- If multiple digits are involved, surgery is staged:
- First stage: release thumb-index and middle-ring fingers.
- Three months later: release index-middle and ring-little fingers.
- First stage: release thumb-index and middle-ring fingers.
- The bifurcation of the digital NVB may be distal to the position of the new webspace.
- Web release is therefore limited to the level of the bifurcation, unless:
- The other side of the finger is not operated on, allowing the bifurcation to be divided.
- There is definitely a second digital artery to supply the finger.
- The other side of the finger is not operated on, allowing the bifurcation to be divided.
- Alternatively, vein grafts can be used to lengthen the artery.
- Web release is therefore limited to the level of the bifurcation, unless:
- The nerve can be separated by interfascicular dissection.
- Linear incisions are avoided due to the risk of scar contracture.
- The web is reconstructed with proximally based dorsal or volar flaps.
- Skin grafts in the web spaces can result in web creep.
- Dorsal and volar interdigitating flaps close defects along the borders of the digits.
- Full thickness skin grafts may be required to resurface residual raw areas.
- Mild first web syndactyly can be released with local flaps, e.g. four-flap Z-plasty.
- Severe syndromal syndactyly may require transposition flaps, tissue expansion or distant/free flaps.
- Hyponychial interdigitating flaps, described by Buck-Gramcko, can reconstruct the lateral nail fold.
- Complications include: vascular compromise, infection, dehiscence, graft loss.
- The commissure may be pulled distally by scar contraction (web creep).
- Scars may cause joint contracture.
- Joint instability, due to insufficient collateral ligaments.
- The normal webspace slopes 45° dorsal to palmar and runs from the metacarpal heads to the midpoint of the proximal phalanx.
Camptodactyly
- From the Greek, meaning ‘bent finger’.
- Characterised by progressive flexion deformity of the proximal interphalangeal joint (PIPJ).
- Often bilateral; most commonly involves the little finger.
- Affects <1%.
- Virtually anything crossing the volar aspect of the finger may cause camptodactyly.
- Most commonly an abnormal lumbrical insertion or short flexor digitorum superficialis (FDS).
- Examining PIPJ extension with the MCPJ alternately flexed and extended can differentiate between intrinsic and extrinsic causes.
- Function is rarely affected; treatment is usually sought for the appearance.
- Bone and joint abnormalities on x-ray are usually secondary changes rather than the primary cause.
Classification
- Type I: presents during infancy; most common type. Most do not require treatment.
- Type II: presents during preadolescence (age 7–11); affects girls more than boys.
- Often progresses to a severe deformity.
- Type III: severe type associated with various syndromes.
Treatment
- The majority of cases with contractures <40° are treated conservatively.
- Involves stretching exercises, splinting and serial casting.
- Difficult to correct surgically.
- Radiological signs that indicate the deformity may be difficult to correct:
- Narrowing of the joint space
- Indentation of the neck of the proximal phalanx
- Flattening of the head of the proximal phalanx.
- Narrowing of the joint space
- Surgical options:
- Exploration and release of any tethering structures.
- FDS tendon transfer to the extensor surface.
- Angulation osteotomy.
- Arthrodesis.
- Exploration and release of any tethering structures.
Trigger thumb
- ‘Congenital’ trigger thumb is a misnomer because it is not found in newborns.
- Also, the thumb does not usually ‘trigger’—it is typically fixed in flexion.
- Prevalence at 1 year is 3 per 1000; bilateral in up to 30%.
- Trigger thumb likely develops with postnatal growth.
- Notta’s nodule is always present.
- May be palpable within flexor pollicis longus (FPL) just proximal to the A1 pulley.
- Trigger finger is less common than trigger thumb.
- The pathology may lie at the A1 pulley and/or at the decussation of FDS.
Treatment
- Observation is reasonable under 1 year of age.
- 30% resolve spontaneously within the first year.
- Joint contractures do not occur if release is delayed until age 3.
- When to operate is agreed between surgeon and parents, considering the risks and benefits.
- Surgical treatment involves release of the A1 pulley.
Clasped thumb
- A spectrum of congenital thumb abnormalities ranging from deficiency of thumb extensor mechanism to more severe problems with thenar muscles and first web contracture.
- Also associated with arthrogryposis.
- Diagnosis often delayed because infants hold thumbs in their palms for the first 3 months.
- Extension lag of the MCPJ differentiates it from trigger thumb.
Treatment
- Goal of treatment is to restore the thumb’s ability to grasp.
- Initial treatment is splintage in extension for up to 6 months.
- Effective when commenced <1 year.
- Surgery indicated if splintage fails, or the child is older than 2 years.
- Adduction contracture requires release of the first web.
- Tendon transfers or grafts to the extensor mechanism for severe deformities that remain passively correctable.
- Joint fusions for malpositioned fixed deformities.
Arthrogryposis
- From the Greek, meaning ‘curved joint’.
- Also known as arthrogryposis multiplex congenita.
- A syndrome of non-progressive joint contractures present at birth.
- Spectrum of severity and many different types, including clasped thumb and windblown hand.
- Most common types occur sporadically; can be part of Freeman–Sheldon syndrome.
- Proposed aetiology is lack of motion during fetal development, leading to joint contractures.
- Can be caused by neuromuscular abnormalities, restricted intrauterine space, vascular insufficiency or maternal illness.
- There may be reduced numbers of spinal anterior horn cells.
- Can be caused by neuromuscular abnormalities, restricted intrauterine space, vascular insufficiency or maternal illness.
Clinical findings
- Congenital contractures, usually symmetrical and bilateral.
- Adduction and internal rotation of the shoulders.
- Elbows fixed in extension with pronated forearms.
- Wrists flexed with the hand in ulnar deviation.
- Flexed and stiff digits.
- Lack of subcutaneous tissue and muscle wasting.
- Thin, waxy skin with no joint creases.
- Lower limb involvement is an important consideration.
Treatment
- Goals of treatment:
- Independent function for feeding and perineal care.
- Maintaining or increasing passive and active motion.
- Preserving bimanual function.
- Independent function for feeding and perineal care.
- A team approach is required, with the help of adaptive equipment.
- Treatment begins early:
- Dynamic and static splintage.
- Passive stretching and range of motion exercises.
- Dynamic and static splintage.
- Surgical intervention is controversial; indicated for specific functional problems:
- Recalcitrant elbow contracture release.
- Restoration of elbow flexion with muscle transfers.
- Examples include partial triceps, pectoralis major or free gracilis.
- Distraction lengthening of wrist soft tissues.
- Dorsal wedge osteotomy of the radius and tendon transfer may allow use of a keyboard.
- Reconstruction of a clasped thumb.
- Recalcitrant elbow contracture release.
Skeletal failures of differentiation
Clinodactyly
- From the Greek, meaning ‘inclined finger’.
- Characterised by curvature of a digit in the radio-ulnar plane.
- Associated with many syndromes, including 25% of Down’s syndrome.
- Most commonly affects the little finger.
- Usually turns the fingertip towards the middle finger.
- The cause is usually deformity of the middle phalanx—often a triangular shaped delta phalanx.
- Formed by a J- or C-shaped epiphysis, which extends onto the lateral side of the phalanx.
- Also known as a longitudinal bracketed epiphysis.
- Formed by a J- or C-shaped epiphysis, which extends onto the lateral side of the phalanx.
- Growth from the longitudinal arm of the epiphysis results in abnormal lateral growth of the bone.
- Kirner’s deformity should not be confused with clinodactyly:
- Progressive palmar-radial curvature of the distal phalanx, usually the little finger.
- Develops in adolescence; can be inherited or occur sporadically.
- Almost never affects function.
- Progressive palmar-radial curvature of the distal phalanx, usually the little finger.
Treatment
- The majority of cases are mild and should be discouraged from surgery.
- Surgery considered if function is limited.
- This should be delayed until skeletal maturity.
- Wedge osteotomy corrects the angulation.
- Usually an opening wedge because the finger is often short.
- Exchange wedge osteotomy inserts the wedge excised from the longer side of the phalanx into an opening wedge osteotomy on the shorter side.
- Usually an opening wedge because the finger is often short.
- Soft tissue shortage may require Z-plasty or local flaps.
- Resection of the epiphyseal bracket with interposition fat graft was described by Vickers.
Symphalangism
- Congenital fusion of one phalanx to another within the same digit.
- Associated with a number of other conditions, including:
- Syndactyly
- Apert’s syndrome
- Poland’s syndrome
- Radial longitudinal deficiency.
- Syndactyly
- Flexion and extension creases over the affected joints are absent.
- Radiological changes:
- Short middle phalanges
- Poorly developed joints and epiphyses.
- Radiological changes:
Treatment
- Managed conservatively with physiotherapy and splintage.
- Osteotomy or arthrodesis is considered once skeletally mature.
Synostosis
- Abnormal fusion of two bones.
- Can occur at any site where two bones are adjacent to one another.
- Synostosis between phalanges occurs in complex syndactyly.
- Carpometacarpal, intercarpal and radiocarpal synostosis seldom require surgery.
- Radio-ulnar synostosis poses functional problems if both forearms are affected.
- Rotational osteotomy through the synostosis is performed around 5 years of age.
- Aims to fix the dominant limb in 10°–20° pronation and the other midprone.
- Allows eating, writing, bimanual manipulation and perineal care.
- Aims to fix the dominant limb in 10°–20° pronation and the other midprone.
Duplication
- Can involve the whole limb or any part of the limb.
- Polydactyly is when more than five digits are present in a hand.
- One of the most common upper limb malformations.
- Extra digits may be located on the ulnar border, centre or radial border.
- One of the most common upper limb malformations.
Ulnar polydactyly
- Also known as postaxial polydactyly.
- Usually an autosomal dominant trait with variable penetrance.
- Often associated with syndromes in Caucasians.
- Other systemic abnormalities should be sought.
- Often bilateral; commoner in boys.
- Incidence is 1:2000 among Caucasians; 1:150 among African Americans.
- Stelling classification of polydactyly:
- Type I: soft tissue mass without skeletal structure.
- Type II: digit contains all normal components and articulates with a normal or bifid metacarpal or phalanx.
- Type III: complete digit with metacarpal.
- Type I: soft tissue mass without skeletal structure.
Treatment
- Type I: excised under local anaesthetic in the first few weeks of life.
- Avoids a residual nubbin resulting from simple ligation.
- Types II and III: surgical excision and reconstruction of soft tissue elements:
- Attachments of the ulnar collateral ligament (UCL) and abductor digiti minimi (ADM) are transferred to the adjacent finger.
Central polydactyly
- Rarest form of duplication; affects the ring finger in most cases.
- Stelling type II variants usually occur with syndactyly.
Treatment
- Types I and III: excision with soft tissue reconstruction.
- Type II synpolydactyly may share tendons, nerves and vessels with adjacent fingers.
- The most suitable skeletal and tendinous elements are selected to create the best digit.
Radial polydactyly
- Refers to duplication of the thumb—preaxial polydactyly.
- Isolated thumb polydactyly is usually unilateral and sporadic.
- Syndromal association is documented but rare.
- Children should be screened for Fanconi’s anaemia.
- Unlike ulnar polydactyly, it affects Caucasians more than African Americans.
- Typically, there is a degree of hypoplasia of both duplicates.
- Neurovascular anatomy is variable; most have only one vessel to each duplicate.
Classification
- Wassell’s classification, with prevalence of each type:
- Type I: bifid distal phalanx (2%)
- Type II: duplicated distal phalanx (15%)
- Type III: bifid proximal phalanx with duplicated distal phalanx (6%)
- Type IV: duplicated proximal and distal phalanx (43%)
- Type V: bifid metacarpal with duplicated proximal and distal phalanx (10%)
- Type VI: duplicated metacarpal, proximal and distal phalanx (4%)
- Type VII: triphalangeal thumb accompanied by a normal thumb (20%).
- Type I: bifid distal phalanx (2%)
Surgical correction
- The goal is to create the best thumb possible using parts of each duplicate:
- A well-aligned thumb with stable joints, balanced motor functions and a cosmetic nailplate.
- Surgery is usually done at 1 year, prior to development of thumb-index pinch.
- In deciding which duplicate to retain, consider:
- Size—occasionally one is rudimentary.
- Deviation—at the point of duplication or at distal joints.
- Function—can differ between duplicates; functions may be shared.
- Flexion in one but extension in the other.
- Passive mobility—both normal and abnormal.
- Radiological appearances—may reveal a triphalangeal thumb.
- Size—occasionally one is rudimentary.
- Surgical options:
- Removing one duplicate and reconstructing the other.
- For types III and IV, or types I and II with significant asymmetry.
- The radial duplicate is usually proximal and smaller than the ulnar.
- Radial collateral ligaments should be reconstructed.
- Usually by taking a periosteal sleeve from the digit to be amputated.
- Intrinsic muscles are reattached in a similar fashion.
- Additional articular facets of the proximal joint surface are excised.
- Improves angular deformity.
- The reconstruction is protected with a transarticular K wire for 4 weeks.
- Principles of treatment are similar for types V and VI.
- More complex reconstruction of the intrinsics is required.
- In addition, first webspace narrowing may need to be addressed.
- More complex reconstruction of the intrinsics is required.
- Removing parts of both duplicates and combining the remaining tissue.
- Symmetric types I and II are treated this way.
- The Bilhaut-Cloquet procedure shares equal parts of each:
- Remove adjacent inner halves of each duplicate.
- The remaining outer segments are brought together and secured with sutures or K wire.
- Remove adjacent inner halves of each duplicate.
- Problems include nail deformity, epiphysiodesis and joint stiffness.
- Proposed modifications involve unequal sharing of parts:
- The entire nail bed is taken from one of the duplicates.
- Bone resection preserves the entire physis and joint surface from one of the duplicates.
- The entire nail bed is taken from one of the duplicates.
- For types III and IV, or types I and II with significant asymmetry.
- Removing one duplicate and reconstructing the other.
Triphalangeal thumb polydactyly
- The duplicate has three rather than two phalanges.
- Relatively common; usually an autosomal dominant trait.
- The extra ‘middle’ phalanx may be:
- Triangular (a delta phalanx)
- Rectangular but short
- Rectangular and normal length.
- Triangular (a delta phalanx)
- Treatment follows the principles above.
- If the triphalangeal duplicate is retained, the extra interphalangeal joint (IPJ) must be addressed:
- Any delta phalanx is excised and soft tissues reconstructed.
- If the extra phalanx is rectangular—chondrodesis of the least mobile joint.
- Any delta phalanx is excised and soft tissues reconstructed.
Mirror hand
- Rare condition—symmetrical duplication of the limb in the midline.
- Quoted incidence of 60 cases per 300 years.
- A central digit with three fingers either side representing middle, ring and little.
- Results in a hand with at least seven fingers but no thumb.
- The forearm has two ulnae (no radius) that support a duplicated ulnar carpus.
- The elbow is usually stiff and forearm rotation reduced.
- The surgical anatomy is variable and complex.
- The elbow is usually stiff and forearm rotation reduced.
Treatment
- Passive stretching and mobilisation of the elbow.
- Fabrication of a first webspace.
- Pollicisation and reducing the number of fingers.
- It is a rarely performed operation, even for congenital hand specialists.
Overgrowth
Macrodactyly
- Enlargement of a digit noted at birth, or within the first years of life.
- True macrodactyly is enlargement of both the soft tissue and skeleton of a finger.
- Aetiology is unknown.
- It is distinct from conditions such as haemangiomas, vascular malformations and Ollier’s disease (multiple enchondromatosis) where overgrowth is due to a specific lesion.
- Macrodactyly is usually unilateral; the index finger is most commonly affected.
- Multiple digits can be involved; can also affect toes.
- Enlargement often corresponds to the cutaneous distribution of specific nerves.
- ‘Nerve territory-oriented macrodactyly’ describes this relationship.
Classification
- Static macrodactyly: the enlarged finger grows in proportion to the rest of the hand.
- Progressive macrodactyly: the enlarged finger grows out of proportion to the rest of the hand.
- Flatt classifies macrodactyly according to the pathology:
- Type I: Lipofibromatosis
- Epineural and perineural fibrosis with fatty infiltration of the nerve.
- Type II: Neurofibromatosis
- Occurs in conjunction with plexiform neurofibromatosis.
- Type III: Digital hyperostosis
- Osteochondral periarticular nodules but no nerve enlargement.
- Type IV: Hemihypertrophy
- Commonly known as Proteus syndrome.
- Type I: Lipofibromatosis
Surgical correction
- Complicated by delayed healing due to relative vascular insufficiency (vessels are rarely enlarged).
- Surgical options are usually inadequate:
- Soft tissue reduction, including digital nerve stripping
- Osteotomy
- Epiphysiodesis
- Amputation.
- Soft tissue reduction, including digital nerve stripping
Undergrowth
Thumb hypoplasia
- Most common site of clinically significant undergrowth.
- Part of radial longitudinal deficiency—associated with the same syndromes.
- Children should be screened for Fanconi’s anaemia.
- Part of radial longitudinal deficiency—associated with the same syndromes.
Classification
- Blauth’s classification has been modified into five groups:
- Type I
- Minor generalised hypoplasia.
- Type II
- Hypoplastic thenar muscles.
- Adduction contracture of the first web.
- Insufficiency of the UCL at the MCPJ.
- Hypoplastic thenar muscles.
- Type III
- Features of type II plus abnormal extrinsic tendons.
- Skeletal abnormalities further subclassify type III (Manske et al.):
- A: stable carpometacarpal joint (CMCJ)
- B: unstable CMCJ.
- A: stable carpometacarpal joint (CMCJ)
- Features of type II plus abnormal extrinsic tendons.
- Type IV
- Small thumb attached to the hand by a soft tissue bridge.
- Known as a floating thumb or ‘pouce flottant’.
- Small thumb attached to the hand by a soft tissue bridge.
- Type V
- Total absence of the thumb.
- Type I
Surgical correction
- Usually done at 1–2 years when thumb function is developing.
- Type I: good function; do not require surgery.
- Type IIIB, IV and V: ablation of any thumb elements and pollicisation.
- Pollicisation is described under ‘Radial deficiency’.
- Type II and IIIA are reconstructed as follows:
- First webspace release with, e.g. four-flap Z-plasty.
- May require release of the first dorsal interosseous from the second metacarpal.
- UCL reconstruction.
- UCL deficiency may be primary or secondary to a pollex abductus.
- This is an abnormal connection between FPL and EPL.
- Any pollex abductus is released and the MCPJ stabilised:
- Chondrodesis (joint fusion), or
- Tendon graft to augment the vestigial UCL, or
- UCL reconstruction incorporated into an FDS opponensplasty.
- Chondrodesis (joint fusion), or
- UCL deficiency may be primary or secondary to a pollex abductus.
- Opponensplasty to augment hypoplastic thenar muscle function.
- Using the ring finger FDS is favoured by many due to its length, power and ability to reconstruct the UCL.
- Others prefer the Huber transfer (ADM to APB).
- Using the ring finger FDS is favoured by many due to its length, power and ability to reconstruct the UCL.
- Extrinsic tendon reconstruction.
- EIP can be transferred to EPL.
- Reconstructing FPL may need pulley reconstruction in addition to tendon transfer.
- EIP can be transferred to EPL.
- First webspace release with, e.g. four-flap Z-plasty.
Brachydactyly
- Brachydactyly (short finger) may occur in isolation, as part of a complex hand anomaly, or other syndrome.
- Often associated with syndactyly, clinodactyly and symphalangism.
Treatment
- Surgery is seldom required—function is relatively well preserved.
- Surgery frequently produces stiff fingers.
- Brachymetacarpia may be corrected by distraction osteogenesis to restore normal cascade.
Madelung’s deformity
- Excessive radial and palmar angulation of the distal radius caused by growth disturbance of the palmar and ulnar portion of the distal radial physis.
- An abnormal palmar ligament may tether the lunate to the radius (Vickers’ ligament).
- Deformity becomes apparent in early adolescence; usually bilateral.
- The distal ulna is prominent dorsally; ulnar deviation of the wrist is limited.
- The forearm is usually short but function is minimally impaired.
- More severe cases may be limited by pain.
- Madelung’s may form part of Leri–Weill dyschondrosteosis, a genetic condition resulting in short stature.
- For this reason it is sometimes classified as a ‘generalised skeletal abnormality’.
Treatment
- No treatment is required for painless deformities.
- Surgery may involve:
- Resection of Vickers’ ligament and dome osteotomy to correct the radius.
- Closing wedge osteotomy of the radius with ulnar shortening.
- Opening wedge osteotomy of the radius.
- Osteotomy of the radius and distal ulnar resection.
- Osteotomy of the radius and a Sauvé–Kapandji procedure.
- This fuses the distal radio-ulnar joint (DRUJ) and resects a segment of ulna to allow forearm rotation.
- Resection of Vickers’ ligament and dome osteotomy to correct the radius.
Constriction ring syndrome
- Constriction rings, or amniotic bands, form partial or complete circumferential constrictions around limbs or digits.
- This can lead to:
- Acrosyndactyly
- Terminal absence or amputation
- Localised swelling with oedema distal to the constrictions.
- Acrosyndactyly
- Occurs sporadically; affects one in 15,000 live births.
- 50% of cases are associated with talipes equinovarus, cleft lip and palate, haemangioma, and cranial or cardiac defects.
- Aetiology may be disruption of the amniotic membrane with release of amniotic bands that encircle limbs in utero.
Classification
- Patterson’s classification:
- Simple constriction rings
- Rings accompanied by distal deformity, with or without lymphoedema
- Rings accompanied by distal fusion: acrosyndactyly
- Intrauterine amputations.
- Simple constriction rings
Surgical correction
- Digital ischaemia at birth is rare.
- Requires surgical release, although the distal limb rarely survives.
- Centres of expertise have released bands fetoscopically.
- Nerve palsies can be difficult to treat because there may not be a distal nerve trunk.
- Treatment of the ring itself is done for cosmesis and function.
- Excision of the constriction band and soft tissue release with Z or W plasties is done for most cases.
- Traditionally, no more than half the circumference was released at one sitting due to risk of distal ischaemia.
- However, complete circumferential release can be performed safely.
- Principles of acrosyndactyly management are similar to syndactyly.
- Intrauterine amputations, in contrast to other congenital causes of absent digits, have intact proximal bone, tendon and neurovascular structures.
- This makes toe transfer an attractive option for restoration of function.
Hand trauma
Assessment
- Identify and treat all immediately life-threatening injuries prior to considering the hand injury.
History
- Hand dominance, occupation, hand-critical hobbies.
- Mechanism of injury and forces involved.
- Time of injury, particularly ischaemia time.
- If machinery is involved:
- Configuration of the moving parts
- How much force it delivers
- What material is normally cut or deformed by the machine
- Are parts of the machine heated and to what temperature?
- Configuration of the moving parts
- If an electrical saw is involved: thickness of the saw blade.
- The direction a knife or shard of glass entered the skin.
- Position of the hand at the time of injury.
Examination
- Is the injured hand or finger viable?
- Vascular injury or compartment syndrome?
- Tendon, nerve or bony injury?
- True skin loss, or impending skin loss?
- Plain X-rays assist with pre-operative assessment.
- Fractures and dislocations present with swelling, deformity and loss of function.
- On palpation, there is tenderness, crepitus and abnormal motion.
- Abnormal motion is also seen with periarticular ligament injury.
- On palpation, there is tenderness, crepitus and abnormal motion.
- Tendons are initially assessed by inspecting the posture of the hand.
- Passive flexion and extension of the wrist can demonstrate tendon integrity by the tenodesis effect.
- However, partial tendon division or isolated FDS division will appear normal.
- Intrinsic muscles can extend IPJs even when extrinsic extensors are divided.
- However, partial tendon division or isolated FDS division will appear normal.
- Active motion of each tendon is then tested independently.
- Composite motion produces the following grip types:
- Power grip
- Pinch grip
- Pure (tip) pinch
- Tripod pinch
- Key (lateral) pinch.
- Pure (tip) pinch
- Power grip
- Nerve injuries present with sensory loss, motor loss or both.
- Sensation is grossly assessed by stroking within a nerve territory and simultaneously comparing with the uninjured hand.
- Sweating is lost in the distribution of a divided peripheral nerve.
- Skin feels smooth and dry.
- The tactile adherence test assesses sweating by lightly dragging the smooth surface of a plastic pen along the skin.
- Skin feels smooth and dry.
- Sensation is assessed more objectively by static and dynamic two-point discrimination (2PD):
- If a specific tool is unavailable, a paper clip can be folded into two points.
- The pressure applied should not result in blanching.
- Guideline values for normal 2PD are:
- Distal phalanx pulp—4 mm
- Middle phalanx pulp—5 mm
- Proximal phalanx pulp—6 mm
- Distal palm—7 mm
- Mid-palm—8 mm
- Proximal palm—9 mm
- Dorsal hand—15 mm
- Volar forearm—25 mm.
- Distal phalanx pulp—4 mm
- If a specific tool is unavailable, a paper clip can be folded into two points.
- Paralysis of APB most reliably indicates median nerve injury.
- Paralysis of FDM most reliably indicates ulnar nerve injury.
- Other intrinsic muscles may be cross-innervated.
- Paralysis of FDM most reliably indicates ulnar nerve injury.
Position of safe immobilisation (POSI)
- Immobilising the hand has the following advantages:
- Pain relief
- Reduction of post-traumatic inflammation and oedema
- Protection of soft tissue repairs
- Splinting of fractures.
- Pain relief
- The POSI, also called intrinsic-plus or Edinburgh position, is:
- Wrist in 0°–30° of extension
- Decreases MCPJ extension by the tenodesis effect.
- MCPJs in 70°–90° of flexion
- Places the collateral ligaments at their maximum length.
- IPJs in full extension
- Prevents volar plate shortening.
- Thumb abducted and pronated
- Prevents first webspace contracture.
- Wrist in 0°–30° of extension
- Splintage is combined with elevation to reduce oedema.
Tourniquets in hand surgery
- Modern tourniquet units are pneumatic and microprocessor-controlled.
Guidelines for safe use
- There is little evidence in support of any guidelines.
- Use the widest cuff possible—wider cuffs occlude at lower pressure.
- Wrinkle-free padding under the cuff minimises risk of skin pinching.
- Avoid aggressive exsanguination for infection or malignancy.
- Suggested maximum inflation pressure for the upper limb is 250 mmHg, or 100 mmHg above systolic blood pressure.
- Suggested maximum inflation time is 2 hours; the evidence ranges from 45 minutes to 4 hours.
- Breaks of 20 minutes allow the venous pH of the limb to normalise between inflations.
Complications of tourniquet use
Local
- Muscle injury
- Mechanical compression by the cuff
- Ischaemia beneath and distal to the cuff
- Reperfusion injury following tourniquet deflation.
- Mechanical compression by the cuff
- Nerve injury
- Most occurs directly under the cuff.
- Disturbance of myelin and nodes of Ranvier due to mechanical pressure.
- Tourniquet-related nerve injury has a reported incidence of 0.1–8%.
- Most lesions recover spontaneously within 6 months.
- Most occurs directly under the cuff.
- Vascular injury
- Rare—thought to occur when atheromatous plaques rupture.
- Skin injury
- Chemical burns—seepage of alcoholic skin preparations beneath the tourniquet.
- Pressure necrosis—inadequate padding or poor application of the tourniquet.
- Chemical burns—seepage of alcoholic skin preparations beneath the tourniquet.
- Tourniquet pain
- Dull aching pain that develops after 10–20 minutes.
- Can occur despite regional anaesthesia, possibly because C fibres are more resistant to local anaesthetic.
- Dull aching pain that develops after 10–20 minutes.
Systemic
- Cardiovascular effects
- Poorly tolerated in patients with little cardiac reserve.
- Limb exsanguination can increase circulating volume by 15%.
- May precipitate cardiac failure.
- Tourniquet release decreases CVP and mean arterial pressure due to:
- Shift of blood back into the limb.
- Release of ischaemic metabolites causing myocardial depression.
- Shift of blood back into the limb.
- Poorly tolerated in patients with little cardiac reserve.
- Pulmonary effects
- Increased end-tidal CO2 following tourniquet release.
- Acute lung injury has been described after limb reperfusion.
- Increased end-tidal CO2 following tourniquet release.
- Neurological effects
- Increased PaCO2 following deflation increases cerebral blood flow.
- Causes reflex decrease in systolic blood pressure, which can critically decrease cerebral perfusion pressure in a brain-injured patient.
- Increased PaCO2 following deflation increases cerebral blood flow.
Replantation and revascularisation
- Replantation is the reattachment of totally amputated parts.
- Revascularisation is the repair of incomplete amputations.
- Macroreplantation
- The amputated part contains muscle bulk and is therefore less resistant to ischaemia.
- Muscle necroses after 6 hours of warm ischaemia or 12 hours of cold ischaemia.
- The amputated part contains muscle bulk and is therefore less resistant to ischaemia.
- Microreplantation
- The amputated parts are usually digits that are more resistant to ischaemia.
- Digits tolerate at least 12 hours of warm ischaemia or 24 hours of cold ischaemia.
- The amputated parts are usually digits that are more resistant to ischaemia.
- The expectations of the patient must be addressed:
- Many choose terminalisation rather than replantation for a shorter recovery time.
Relative indications
- Thumb
- Multiple digits
- Amputation through the palm
- Almost any part in a child
- Wrist, forearm, elbow and above elbow
- Single digit distal to the FDS insertion
- Patients who ‘must’ have a 10-digit hand, e.g. musicians.
Relative contraindications
- Severely crushed or mangled parts
- Avulsion injuries with structures dangling from the part associated with:
- The ‘red streak sign’—bruising over the neurovascular pedicle.
- The ‘ribbon sign’—a corkscrew appearance to the vessels.
- The ‘red streak sign’—bruising over the neurovascular pedicle.
- Amputations at multiple levels
- Extreme contamination
- Previous injury of the amputated part
- Other serious injuries or diseases
- Severe atherosclerosis
- Prolonged ischaemia time
- Mental instability
- Single digit proximal to the FDS insertion.
Ring avulsions
- Classified by Urbaniak et al.
- Class I: Circulation adequate.
- Class II: Circulation inadequate. Microvascular reconstruction will restore circulation and function.
- Class III: Complete degloving or complete amputation.
- Class I: Circulation adequate.
- Class III amputations, particularly proximal to the FDS insertion, have poor prognosis and are best terminalised.
- Others have subdivided class II injuries:
- IIA: Only digital arteries require repair.
- IIB: Arteries, bone, tendon or nerves are involved.
- IIC: Only veins are involved.
- IIA: Only digital arteries require repair.
- Replantation may be attempted distal to the FDS insertion if the PIPJ and proximal phalanx are intact.
Transportation of the amputated parts
- Aim to keep the part cool, prevent freezing and avoid maceration.
- This can be achieved by:
- Wrapping the part in moist gauze and placing it in a sealed container or bag.
- This is then placed in another container or bag containing ice and water.
- Wrapping the part in moist gauze and placing it in a sealed container or bag.
Surgical treatment
- Two surgical teams greatly shorten the operative time.
Team 1
- Osteosynthesis is planned based on X-rays of the hand and amputated part.
- The part is debrided and neurovascular structures tagged in theatre.
- Longitudinal midaxial incisions give good exposure.
- Bone shortening may allow primary repair of neurovascular structures.
- The distal half of the bony fixation can be inserted into the amputated part in advance.
- Common methods of fixation:
- K wires
- Interosseous wires
- Miniplates and screws.
- Common methods of fixation:
Team 2
- Debride the stump and tag neurovascular structures.
- Shorten and fix the bone.
- Repair the extensor and flexor tendons.
- Anastomose the arteries, coapt the nerves, then anastomose the veins.
- Skin cover.
- Interposition vein grafts or vessel transposition from an adjacent finger may be required.
- Grafts from the volar wrist match the calibre of digital arteries.
- Grafts can be placed extra-anatomically to the radial artery at the wrist.
- Grafts from the volar wrist match the calibre of digital arteries.
- If suitable veins are not available, venous drainage may be achieved by:
- Repairing any volar veins.
- Anastomosing a digital artery (which has backflow) to a vein, creating an arteriovenous fistula.
- Removing the nail plate and scraping the sterile matrix to encourage bleeding with heparin-soaked gauze.
- Stab incisions of the periungual area and topical heparin.
- Medical leeches.
- Repairing any volar veins.
Special considerations in macroreplantation
- The priority is establishing arterial inflow to minimise muscle necrosis.
- Achieved by a temporary vascular shunt, such as a Sundt, Pruitt-Inahara or Javid shunt.
- Considerable bone shortening is required if amputated through muscle bellies.
- Shortening also makes primary vessel and nerve repair easier.
- Fixation of bone is then done, prior to definitive arterial repair.
- Venous blood is drained from the amputated part for some time to flush accumulated toxic metabolites.
- Blood transfusion is usually required.
- Fasciotomies are always indicated.
- Assess for further muscle necrosis within 48–72 hours under general anaesthesia.
Fingertip injuries
Nail bed injury
- Usually caused by doors in children and DIY tools in adults.
- All require X-ray because 50% have an underlying fracture.
Classification
- Subungual haematoma
- Simple lacerations
- Stellate lacerations
- Severe crush
- Avulsion.
Treatment
- Haematoma with intact nail edges is treated by trephination of the nail.
- Disrupted nailplates are removed to allow assessment of the nail bed.
- Lacerations are approximated with fine dissolving sutures or skin glue.
- Nail bed avulsions can be replaced as grafts.
- Central defects can be repaired directly after paronychial releasing incisions.
- Split thickness nail bed graft from an adjacent finger or toe can be used for defects >30% of the width.
- Associated distal phalanx fractures are normally reduced by approximation of the nail bed, and splinted by application of the nailplate.
- If the fracture is unstable, K wires may be used.
- Disrupted nailplates are removed to allow assessment of the nail bed.
Fingertip amputation
- Optimal management is controversial.
- Reasonable attempts should be made to preserve the length of the thumb.
Classification
- Many systems are available, notably proposed by Tamai, Ishikawa and Allen.
- Allen’s classification:
- Type I: pulp only.
- Type II: pulp and nail bed.
- Type III: distal phalanx fracture with associated pulp and nail loss.
- Type IV: lunula, distal phalanx, pulp and nail loss.
- Type I: pulp only.
Treatment
- The amputated part can be replaced as a composite graft.
- Most successful in children <3 years old when replaced within 5 hours.
- If replantation or composite grafting is not possible or not indicated:
Healing by secondary intention
- Considered by many to be the best option when bone is not exposed.
- Exposed bone can be shortened to allow healing to occur.
Skin grafting
- Studies show superior results are obtained by allowing the wound to heal.
Local and regional flaps
- Prior to flap surgery, the surgeon should be satisfied that the outcome will be superior to bone shortening and healing by secondary intention.
- Rates of cold intolerance and altered sensation are similar with both treatments.
- Options include:
- Atasoy-Kleinert volar V-Y
- Kutler lateral V-Y
- Segmüller lateral V-Y
- Homodigital island
- Venkataswami advancement
- Evans step advancement
- Cross-finger
- Thenar.
- Atasoy-Kleinert volar V-Y
- Tension on the nail bed is avoided during inset to avoid a hook nail.
- Many advocate resecting the nail bed if <25% remains
- Nail spikes and cysts can result if the nail bed is not completely excised.
- Many advocate resecting the nail bed if <25% remains
Thumb reconstruction
- Thumb reconstruction should address:
- Sensation
- To allow interaction with the environment
- Protection
- Freedom from pain.
- To allow interaction with the environment
- Opposition
- Length
- Stability
- Strength
- Mobility.
- Length
- Sensation
- Loss of the distal phalanx may not lead to functional problems.
- Amputation proximal to the shaft of the proximal phalanx is inadequate for pinch and power grip.
Classification
- Lister has rationalised thumb defects:
- Acceptable length with poor soft tissue cover.
- Subtotal amputation with questionable remaining length.
- Total amputation with preserved CMCJ.
- Total amputation with loss of the CMCJ.
- Acceptable length with poor soft tissue cover.
Treatment
- Treatment is dictated by Lister’s classification:
Acceptable length with poor soft tissue cover
- Healing by secondary intention.
- Revision amputation.
- V-Y advancement flaps, as described for fingertip injuries.
- Moberg volar advancement flap.
- Innervated cross-finger flap.
- First dorsal metacarpal artery (FDMA) flap (Foucher, 1979).
- Littler heterodigital island flap.
Subtotal amputation with questionable remaining length
- Deepening the first webspace to relatively lengthen the stump.
Total amputation with preserved CMCJ
- Free toe transfer is ideal.
- Alternatively:
- Metacarpal distraction lengthening.
- Osteoplastic reconstruction (bone graft covered with soft tissue flap).
- Pollicisation of an injured or partially amputated digit.
- Metacarpal distraction lengthening.
Total amputation with loss of CMCJ
- Pollicisation.
Toe-to-hand transplantation
- The aim is to provide a thumb and two fingers for tripod pinch.
Anatomy
- Most transfers are based on the lateral digital artery to the great toe, or medial digital artery to the second toe.
- Toe digital arteries arise from two systems:
- Dorsal arterial system, from dorsalis pedis.
- Plantar arterial system, from plantar metatarsal arteries.
- Dorsal arterial system, from dorsalis pedis.
- Determining which system is dominant is key when harvesting a toe.
- First dorsal metatarsal artery is dominant in 70%.
- First plantar metatarsal artery is dominant in 20%.
- In 10%, both systems are of equal calibre.
- First dorsal metatarsal artery is dominant in 70%.
- Most are harvested with the superficial dorsal venous system.
- Plantar sensation is supplied by plantar digital nerves.
Variants of toe transfer
Great toe transfer
- Used to reconstruct a thumb.
- The donor site may be unacceptable to some patients.
Wraparound technique
- Uses the great toenail, skin envelope and bone graft.
- Gives a smaller thumb than conventional great toe transfer.
- Does not restore joint mobility.
- Not used in children due to the lack of capacity for growth.
Trimmed great toe transfer
- Combines the advantages of toe transfer and wraparound technique.
- Harvested like a conventional great toe transfer.
- Longitudinal osteotomy removes a strip of bone from the side of the phalanges.
- Soft tissue is excised from the medial side to match the intact thumb.
Second toe transfer
- Used following finger amputations.
- Can reconstruct a thumb for those who prefer the donor site to that of the great toe.
- Disadvantages: tendency to claw, bulky pulp.
- Can reconstruct a thumb for those who prefer the donor site to that of the great toe.
Second toe wraparound transfer
- For distal soft tissue loss of the fingers.
- The distal phalanx is included to prevent pulp instability and nail deformity.
Third toe transfer
- Rarely used; indicated if a second toe is not available.
Combined toe transfer
- Useful if two adjacent digits are required.
- Combinations of second-third or third-fourth toes can be transferred.
- Provides a webspace, and both toes are supplied by a shared pedicle.
Vascularised joint transfer
- Indicated for a destroyed PIPJ or MCPJ.
- Limited range of motion, but is stable, durable and shows capacity for growth.
- Usually harvested from the second toe, based on articular branches from the medial digital artery.
Neurosensory free flaps
- Useful for large pulp defects that cannot be reconstructed with local flaps.
- Free pulp flaps from the great toe provide potentially sensate glabrous skin from a donor site that is closed primarily.
- First webspace flaps are thin, potentially sensate islands of glabrous skin.
Donor site
- Sequelae of toe harvest should be discussed in detail with patients.
- Photographs of feet following toe harvest should be shown.
- The donor site should be closed primarily with minimal tension.
- Most patients do not have problems walking.
- Some experience fatigue when playing ball sports.
Fractures and dislocations
Collected words of wisdom
- There is a wide range of acceptable treatment.
- Little evidence supports superiority of one method over another.
- Treat fractures using methods that work for you.
- Some eminent hand surgeons treat almost all fractures non-operatively.
- Others treat almost all fractures operatively, with similar results.
- Some eminent hand surgeons treat almost all fractures non-operatively.
- Surgery causes bleeding, swelling, scarring, and implants can become infected.
- Operative treatment can therefore result in worse outcomes than no treatment.
- More aggressive surgery generally attracts more spectacular complications.
- First do no harm—do not operate unless you can provide a superior outcome to non-operative management.
- Oedema causes stiffness—elevate the fractured limb above heart level.
- First do no harm—do not operate unless you can provide a superior outcome to non-operative management.
Principles of fracture management
Assessment
- Identify and treat immediately life-threatening injuries prior to considering the hand fracture.
- Assessment should answer these specific fracture-related questions:
- Is there a wound communicating with the fracture?
- Is there evidence of neurovascular injury?
- Is there evidence of associated soft tissue injury, e.g. tendon or ligament?
- Is there a wound communicating with the fracture?
Investigation
- Most hand fractures are adequately imaged with plain X-ray.
- Complex intra-articular fractures may require a CT scan.
- Ultrasound and MRI assess soft tissue detail.
Treatment
- The three fundamental principles of fracture treatment are:
- Reduction
- By closed manipulation
- By mechanical traction
- By open surgery.
- By closed manipulation
- Minimal displacement or displacement of no functional consequence do not need reduction.
- Translation is generally better tolerated than angulation or rotation.
- Immobilisation
- To prevent displacement of the fragments.
- To prevent movement that might interfere with bone union.
- To relieve pain.
- To prevent displacement of the fragments.
- Immobilisation can be achieved by:
- External splint, e.g. plaster of Paris or Zimmer splint
- Continuous traction
- External fixation
- Internal fixation.
- External splint, e.g. plaster of Paris or Zimmer splint
- Indications for fixation include:
- Irreducible fractures, particularly if malrotated
- Intra-articular fractures
- Subcapital fractures of the phalanges
- Open fractures
- Segmental bone loss
- Polytrauma with hand fractures
- Multiple hand or wrist fractures
- Fractures with soft tissue injury (vessel, tendon, nerve, skin).
- Irreducible fractures, particularly if malrotated
- Methods of internal fixation include:
- K wires
- Interosseous wires
- Intramedullary devices
- Screws
- Plates.
- K wires
- Rehabilitation
- Rehabilitation is required for all fractures.
- Begin as soon as possible, with supervision from a hand therapist.
- Aims of rehabilitation:
- Preserve hand function during fracture union.
- Return hand function to normal once the fracture has united.
- Preserve hand function during fracture union.
- It is unusual to immobilise a hand fracture for more than 3–4 weeks.
- Prolonged immobilisation leads to stiffness.
- Rehabilitation is required for all fractures.
- Reduction
Complications of fractures
Early
- Neurovascular and other soft tissue injury.
- Compartment syndrome.
Late
- Delayed union
- Non-union
- Malunion
- Joint stiffness and contractures
- Avascular necrosis
- Complex regional pain syndrome
- Osteomyelitis
- Growth disturbance or deformity
- Osteoarthritis (OA).
Open surgical approaches to hand fractures
- General aims:
- Provide adequate exposure
- Preserve the skin’s blood supply
- Be extendable if necessary
- Avoid scar contracture.
- Provide adequate exposure
Dorsal approach
- Often used for metacarpals and phalanges.
- Over the DIPJ they can be shaped like an H, Y or L.
- Dorsal veins and sensory nerves are preserved if possible.
- The extensor tendon can be retracted over the metacarpal.
- Juncturae tendinum may need to be divided, but should be repaired.
- Over the proximal phalanx the central slip is freed on one side and retracted.
- Alternatively, the central slip is split longitudinally.
- The Chamay approach is a V-shaped incision through the extensor, allowing the central slip to be reflected distally.
- Gives excellent exposure of the head of the proximal phalanx.
- Requires skill to repair the central slip to avoid extensor lag and boutonnière.
- The extensor tendon can be retracted over the metacarpal.
Lateral approach
- Midaxial incision connects the centres of rotation of the IPJs.
- Surface markings are the dorsal extremes of the IPJ flexion creases.
- The digital NVB is volar to this incision.
- Surface markings are the dorsal extremes of the IPJ flexion creases.
- Midlateral incision is halfway between the dorsal and volar surfaces.
- It is slightly volar to the midaxial line.
- The midaxial incision is generally preferred because it is ‘mechanically neutral’.
Volar approach
- Few closed fractures are approached from the volar aspect.
- Those that are include:
- Volar plate avulsion fracture of the middle phalanx base.
- MCPJ collateral ligament avulsion fracture of the base of the proximal phalanx.
- The collateral ligament travels from the metacarpal to the volar base of the proximal phalanx.
- Volar plate avulsion fracture of the middle phalanx base.
Metacarpal fractures
- Rotational alignment is confirmed by asking the patient to make a fist.
- Fingers should all point to the scaphoid tubercle.
- If the fracture is stable, it is held for 3–4 weeks until union takes place.
- Methods of non-operative fixation include:
- Buddy strapping to an adjacent non-injured finger
- Bedford gaiter
- Plaster of Paris, aiming for 3-point fixation, e.g. ulnar gutter, Barton short hand cast, clam-digger cast.
- Buddy strapping to an adjacent non-injured finger
- Operative treatment is indicated for open fractures.
- Some surgeons also elect to internally fix closed fractures.
- Fixation can be achieved by:
- K wires: transverse, longitudinal, ‘bouquet’ wiring.
- Lag screws
- Plates—newer low profile implants rarely require removal
- Interosseous wires
- External fixation.
- K wires: transverse, longitudinal, ‘bouquet’ wiring.
Fifth metacarpal neck fractures
- So-called boxer’s fracture; often over-treated.
- Well tolerated due to mobility of the CMCJs.
- Rarely requires treatment unless rotated or angulated >70°.
- Usually impacted and stable if left unreduced.
- Patients are told to mobilise their fingers immediately as pain allows.
- A Bedford gaiter or buddy strapping prevents significant extensor lag.
- No follow-up is required.
- Well tolerated due to mobility of the CMCJs.
Phalangeal fractures
- Rotational malalignment must be corrected.
Distal phalanx
- Shaft fractures usually splinted; can be K wired if grossly unstable.
- Bony mallet injuries: splint for 6 weeks.
- Others advocate intervention if >30% of the articular surface is involved, but this is arbitrary.
- Operative fixation is indicated if the DIPJ is subluxed in a splint.
- Others advocate intervention if >30% of the articular surface is involved, but this is arbitrary.
Phalangeal shaft
- Most can be treated conservatively; some elect to treat them operatively.
- Fixation should avoid the IPJs so they can be mobilised.
- K wires are popular—phalanges are easily accessed percutaneously.
Intra-articular fractures
- Aim of treatment is to restore joint congruity and subsequently:
- Prevent deformity
- Prevent OA
- Restore early movement.
- Prevent deformity
- Should be fixed with absolute stability if possible.
- Some fractures require detailed assessment with pre-operative CT.
- Unicondylar fractures of the phalanges are inherently unstable.
- They require anatomical reduction.
- Management is rarely successful with external splintage.
- Percutaneous lag screws or K wires may be possible.
- Otherwise open reduction is required.
- They require anatomical reduction.
- Pilon fractures are comminuted intra-articular fractures.
- Common at the base of the middle phalanx.
- Result from axial loading—the head of the proximal phalanx is driven into the base of the middle phalanx.
- Pilon is the French word for pestle (a heavy tool with a rounded end)
- The articular surface may be splayed.
- Outcome is unpredictable; stiffness is expected.
- For this reason, some favour dynamic external fixators over open reduction and internal fixation (ORIF):
- Examples: Hynes–Giddins device (K wires only) and Suzuki frame (K wires and rubber bands).
- Common at the base of the middle phalanx.
- ORIF usually requires bone graft to support the reduced articular fragments.
- No method can repair the articular surface to its pre-injury state.
Dislocations and subluxations
DIPJ
- Dislocations or subluxations are rare.
- May be associated with avulsions of FDP or extensor tendon.
- Integrity of the collateral ligaments is assessed after ring block.
- Most (without tendon avulsion) are splinted for two weeks, then mobilised.
PIPJ
- Often missed or poorly treated; a great source of litigation.
- Eaton classifies volar plate injuries of the PIPJ as follows:
- Type I (hyperextension)
- Avulsion of the volar plate without fracture; collateral ligaments split.
- Type II (dorsal dislocation)
- Complete dorsal dislocation; volar plate avulsion without fracture.
- Type III (fracture subluxation)
- Fracture subluxation with a palmar fragment of variable size.
- Type I (hyperextension)
- Palmar fragments <40% of the articular surface should leave enough collateral ligament attached to the middle phalanx to provide joint stability when reduced.
- Larger palmar fragments suggest the joint may re-sublux following reduction.
- The ‘dorsal V sign’ on lateral X-ray indicates a subluxed joint.
- Treatment: reduction and early mobilisation in an extension block splint.
- Other options include transarticular K wire, ORIF of the palmar fragment or dynamic external fixator, e.g. Suzuki frame.
MCPJ
- Rare and easily missed.
- Closed reduction may be impossible:
- The volar plate can flip into the joint.
- FDP, FDS and lumbricals form a ‘noose’ around the metacarpal neck.
- The volar plate can flip into the joint.
- Open reduction requires particular care not to injure the digital nerves.
CMCJ
- Uncommon in the radial four rays; indicative of high energy trauma.
- Fifth CMCJ dorsal subluxation is relatively common.
- Results from axial force on the fifth metacarpal.
- Fracture of the metacarpal base is nicknamed a ‘reversed Bennett’s fracture’.
- There may also be a dorsal avulsion from the hamate.
- Results from axial force on the fifth metacarpal.
- Treatment options include:
- Closed reduction and splint
- Closed reduction and K wire into an adjacent metacarpal or carpus
- ORIF.
- Inadequate or lost reduction leads to weak grip.
- Closed reduction and splint
Thumb fractures
- More forgiving due to the greater range of motion in thumb joints.
- Specific thumb fractures include:
Bennett’s fracture–subluxation
- Fracture–subluxation of the first carpometacarpal joint.
- Does not refer to all fractures in the region of the first metacarpal base.
- Mechanism of injury is axial loading of the flexed CMCJ.
- The palmar oblique (‘beak’) ligament holds the fragment in the anatomical position.
- The remainder of the metacarpal is adducted and supinated by adductor pollicis.
- Also pulled proximally by APL.
- The palmar oblique (‘beak’) ligament holds the fragment in the anatomical position.
- The fracture–subluxation is reduced by a combination of:
- Longitudinal traction
- Pronation of the metacarpal
- Pressure at the base of the metacarpal.
- Longitudinal traction
- The reduction can be held by applying a moulded below-elbow cast.
- Persistent instability can be held with percutaneous K wires:
- Transfixion of the metacarpal base to the trapezium.
- Transfixion of the first metacarpal base to the second metacarpal.
- Combination of both.
- Transfixion of the metacarpal base to the trapezium.
- ORIF is indicated for irreducible fractures.
- Not usually feasible if the fragment is <20% of the articular surface.
Rolando fracture
- Three-part intra-articular fracture of the base of the first metacarpal.
- Mistakenly used to describe all comminuted fractures of the first metacarpal base.
- Non-operative treatment is unlikely to reduce the articular surface.
- ORIF with a T-plate is usually done through a dorsal or radiopalmar approach.
- More comminuted ‘Rolando’ fractures are difficult to ORIF.
- External fixation can maintain a reasonable reduction and prevents metacarpal collapse.
- Rolando fractures are often more comminuted than shown on X-ray.
- Some therefore routinely assess these injuries with CT scan.
MCPJ UCL avulsion
- Frequently missed, leading to instability and weakness of pinch.
- Commonly seen in skiers that fall onto their thumbs (especially while holding a ski pole).
- Colloquially known as ‘skier’s thumb’.
- ‘Gamekeeper’s thumb’ refers to chronic attenuation of the UCL.
- Colloquially known as ‘skier’s thumb’.
- The avulsed ligament can displace dorsal to the adductor aponeurosis.
- Known as a Stener lesion.
- The interposed adductor aponeurosis eliminates any chance of spontaneous bony or ligamentous healing.
- Incomplete injuries are managed conservatively in a cast for 4–6 weeks.
- Complete injuries increase the likelihood of a Stener lesion, requiring surgical repair.
- Stress testing of the UCL is done with the MCPJ in 30° of flexion.
- Comparing with the uninjured side, >15° difference or a soft end-point suggests complete rupture.
- The UCL can be reattached using a Mitek bone anchor.
- Repair is protected for 4 weeks; activity is gradually increased thereafter.
- Known as a Stener lesion.
Paediatric hand fractures
- The vast majority can be managed non-operatively.
- The presence of a physis means that deformity can be remodelled with growth.
- Greatest remodelling potential is seen with the following:
- When angulation occurs in the plane of adjacent joint motion.
- When the fracture is in close proximity to the physis.
- When the fracture is in a young child with many years of remaining growth.
- When angulation occurs in the plane of adjacent joint motion.
- Rotational and angular deformity has little remodelling potential.
- The physis should be respected during surgery.
- Salter–Harris classification of physeal fractures:
- Type I—fracture through the physis (6%)
- Type II—fracture through the physis and metaphysis (75%)
- Type III—fracture through the physis and epiphysis (8%)
- Type IV—fracture through the epiphysis, physis and metaphysis (10%)
- Type V—fracture compressing the physis (1%)
- Type I—fracture through the physis (6%)
- Types III, IV and V are associated with physeal growth arrest.
- Specific paediatric hand fractures include:
Seymour fracture
- Looks like a mallet ‘drop finger’, but is transepiphyseal rather than transarticular.
- Usually open with nail bed involvement.
- The fracture is distracted by the extensor tendon on the proximal fragment and FDP on the distal fragment.
- Requires debridement, reduction, nail bed repair and replacement of the nailplate as a splint.
- An axial transarticular K wire can be passed if unstable.
Phalangeal neck fractures
Related posts:

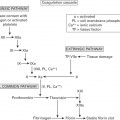
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


