Chapter 4
The Breast and Chest Wall
- Breast anatomy
- Breast reduction
- Mastopexy
- Breast augmentation
- The tuberous breast
- Gynaecomastia
- Breast cancer
- Breast reconstruction
- Chest wall reconstruction
- Posterior trunk reconstruction
- Further reading
Breast anatomy
- The breast base extends vertically from 2nd–6th rib.
- Horizontally, it extends from the lateral margin of sternum to anterior axillary fold.
- The axillary tail of Spence extends superolaterally towards the axilla.
- Each breast contains 15–20 lobes, which radiate outward from the nipple.
- A lobe contains a variable number of lobules; each contains 10–100 alveoli.
- Each alveolus has a small duct that joins with others to form a single duct for each lobule.
- This duct system opens onto the nipple as lactiferous ducts.
- Most breast cancers originate from this ductal system.
- Adjacent lobes are separated by fibrous septa from skin to pectoral fascia.
- Septa in the upper breast are well developed, known as suspensory ligaments of Astley Cooper.
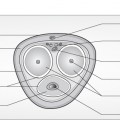
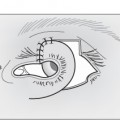
- The thin horizontal fibrous septum of Würinger originates from pectoral fascia along the fifth rib and curves upwards into vertically oriented medial and lateral ligaments.
- This septum attaches the breast to the sternum and lateral edge of pectoralis minor.
- Carries the main nerve supply to the nipple together with intercostal perforators.
- Horizontally, it extends from the lateral margin of sternum to anterior axillary fold.
Arterial supply
- Internal mammary artery perforators
- Pectoral branches of the thoracoacromial axis
- Lateral thoracic artery
- Lateral branches of 3rd–5th intercostal arteries.
Nerve supply
- Anterior cutaneous branches of 2nd–6th intercostal nerves.
- Anterior cutaneous branches of 3rd–6th lateral cutaneous nerves.
- Supraclavicular branches of cervical plexus.
- Main supply to the nipple is from branches of the 4th lateral cutaneous nerve.
Surface anatomy
- Penn described ‘ideal’ breast measurements:
- Sternal notch to nipple distance is roughly equivalent to the distance between the nipples.
- This is 21 cm on average.
- Nipple to inframammary crease is approximately 6.8 cm.
- Areolar diameter varies from 3.8 to 4.5 cm.
- Sternal notch to nipple distance is roughly equivalent to the distance between the nipples.
Brassiere size
- Estimating bra size is difficult: sizes vary between countries and manufacturers.
- This mathematical method of bra sizing is a guide at best.
Band size
- In the United Kingdom, this is based on chest circumference:
- Measured in inches at the inframammary fold (IMF).
- Either 4 or 5 inches are added to make an even number.
- Band sizes typically range from 28 to 46 inches.
- Measured in inches at the inframammary fold (IMF).
Cup size
- Based on the difference between band size and chest circumference around the most prominent part of the breasts:
- <1 inch difference—AA cup
- 1 inch difference—A cup
- 2 inch difference—B cup
- 3 inch difference—C cup
- 4 inch difference—D cup
- 5 inch difference—DD cup.
- <1 inch difference—AA cup
Breast reduction
History
- Thorek (1920s): free nipple graft technique.
- Wise (1950s): keyhole pattern of skin incision.
- Strombeck (1960): horizontal bipedicle technique.
- Skoog (1963): modified Strombeck; superomedial pedicle technique.
- McKissock (1972): vertical bipedicle technique.
- Weiner (1973): superior pedicle technique.
- Ribeiro (1975): inferior pedicle technique.
- Lejour popularised the vertical scar technique originally described by Lassus.
- Benelli (1990): round-block technique.
- Hall-Findlay (1999): modified the vertical scar technique with a medial pedicle.
- Hammond (1999): short scar periareolar inferior pedicle reduction (SPAIR) technique.
- Hamdi (2005): uses the septum of Würinger to maintain vascularity and sensation to the nipple–areola complex (NAC).
- Weiner (1973): superior pedicle technique.
Techniques
- Classified by:
- Pattern of skin excision
- Design of NAC pedicle.
- Pattern of skin excision
Patterns of skin excision
- Wise pattern, also known as a ‘keyhole’ due to its shape.
- Alternatively known as an ‘inverted T’ due to the resultant scars.
- Regnault described a ‘B’-shaped skin excision.
- Lejour popularised vertical skin excision.
- Marchac described vertical excision with short lateral extensions.
- Benelli popularised the periareolar technique.
Design of the pedicle
- Blood reaches the NAC via a pedicle from the chest wall, composed of:
- Glandular tissue, or
- Glandular tissue and de-epithelialised dermis, or
- Horizontal septum of Würinger.
- Glandular tissue, or
Free nipple graft technique
- The NAC is removed and replaced as a graft.
- Advantages:
- Avoids morbidity associated with a long pedicle.
- Relatively quick and easy to perform.
- Avoids morbidity associated with a long pedicle.
- Disadvantages:
- Poor ‘take’ of the NAC.
- Loss of nipple sensation.
- Poor ‘take’ of the NAC.
- For these reasons, the technique is generally reserved for older patients requiring large reductions.
Inferior pedicle technique
- Popular technique of breast reduction.
- Advantages:
- Relatively simple to learn.
- May preserve nipple sensation via the 4th lateral cutaneous nerve.
- Relatively simple to learn.
- Key points of the inferior pedicle technique:
- The pedicle must remain attached to the chest wall.
- Avoid undermining the pedicle.
- The base of the pedicle can be inclined laterally.
- Increases the chance of including a sensory branch in the pedicle.
- In firm breasts, the width of the keyhole pattern should be narrowed.
- Otherwise undue tension may be placed on the skin flaps.
- The NAC should never be sited too high.
- A high nipple is difficult to correct.
- At the end of the procedure, the nipples should lie just below the most prominent part of the breast.
- A high nipple is difficult to correct.
- The pedicle must remain attached to the chest wall.
Medial pedicle technique
- Also a popular technique of breast reduction.
- With the patient upright it looks like more of a superomedial pedicle.
- The Hall-Findlay technique combines it with vertical skin excision.
- Key technical points:
- Create a full thickness dermoglandular pedicle down to chest wall, without exposing pectoralis fascia.
- Parenchymal resection predominantly inferiorly and laterally.
- The inferior border of the pedicle becomes the medial breast pillar after the nipple is rotated into position.
- Pillars are sutured together to cone the breast; skin redrapes over the parenchyma.
- Create a full thickness dermoglandular pedicle down to chest wall, without exposing pectoralis fascia.
Mastopexy
- Corrects ptosis by elevating breast tissue and NAC.
- Ptosis is derived from the Greek, meaning ‘to fall’.
- Involves excision of breast skin without parenchymal resection.
Classification
- Regnault classified breast ptosis:
First degree ptosis
- Nipple lies at the level of the IMF, above the lower contour of the gland and skin brassiere.
Second degree ptosis
- Nipple lies below the IMF but above the lower contour of the breast and skin brassiere.
Third degree ptosis
- Nipple lies below the IMF and at the lower contour of the breast and skin brassiere.
Pseudoptosis
- The major portion of the breast mound lies below the IMF while the NAC remains at the level of the IMF.
- This appearance can occur after breast reduction.
Surgical correction of ptosis
Augmentation only
- An implant can increase breast volume and improve contour.
- Can treat minor degrees of ptosis.
- Not suitable for more severe ptosis because:
- An excessively large implant would be required to tighten the slack skin.
- Ptotic skin may hang over the implant creating a ‘double-bubble’ or ‘Snoopy-nose’ appearance.
- An excessively large implant would be required to tighten the slack skin.
Skin excision and glandular remodelling
- Four main scar patterns:
Periareolar technique
- Involves de-epithelialising a concentric ring of tissue around the NAC.
- Breast skin is tightened by suturing the outer ring to the NAC.
- Benelli described a ‘round-block’ technique of securing the NAC after circumareolar mastopexy:
- A purse-string (the ‘round-block’) reduction of the outer dermal circumference with a permanent suture.
- A ‘skin compensation suture’: horizontal bites of the outer dermal circumference, but vertical bites of the NAC.
- A purse-string (the ‘round-block’) reduction of the outer dermal circumference with a permanent suture.
- Advantages:
- Reduces the tendency of the NAC to stretch.
- Reduces the tendency of nipple herniation through the ‘round-block’.
- Minimises puckering as a larger circle is closed to a smaller diameter NAC.
- Reduces the tendency of the NAC to stretch.
Vertical scar technique
- Adds a vertical or oblique limb to the periareolar skin excision:
- Allows more skin to be excised.
- Helps elevate the NAC.
- Allows more skin to be excised.
Inverted T scar technique
- The full Wise ‘keyhole’ pattern is used for severe ptosis:
- Removes large amounts of excess skin.
- Transposes the NAC into its correct position.
- Removes large amounts of excess skin.
L-shaped scar technique
- Reduces the length of the horizontal component of the inverted T technique by eliminating the medial component and shortening the lateral component.
- Best suited to correcting first or second degree ptosis.
Complications of mastopexy and breast reduction
General
- Risks of general anaesthesia
- Chest infection and atelectasis
- Deep vein thrombosis or pulmonary embolism
Specific
Early
- Altered nipple sensation (20%)
- Haematoma (1%)
- NAC necrosis (<0.5%)
- Infection.
Intermediate
- Wound healing problems (5%)
- Seroma
- Fat necrosis.
Late
- Inability to breastfeed (up to 50%)
- Hypertrophic or keloid scarring
- Lumpiness
- Under- or over-resection
- Asymmetry
- Dog ears.
Breast augmentation
History
- 1890: breasts augmented with paraffin wax injections.
- 1950: polyvinyl sponge implants available.
- 1960s: silicone gel prosthetic augmentation first performed by Cronin and Gerow.
- Estimated that 3% of women in the United States have undergone breast augmentation.
- In the United Kingdom, >10,000 women had breast implants for cosmetic purposes in 2011.
Classification
- Implant-based breast augmentation can be classified by:
- Composition and surface of the implant shell
- Contents of the implant
- Implant shape
- Incision through which the implant is inserted
- Site of implant placement.
- Contents of the implant
- Composition and surface of the implant shell
Implant shell
Texture of the shell
- Smooth
- Textured
- Believed to induce less capsular contracture.
Composition of the shell
- Most breast implant shells are silicone.
- Polyurethane foam coated implants are increasing in popularity.
- Reported to have lower rates of capsular contracture.
- Concerns over formation of toluene by-products (carcinogenic in animals) resulted in their temporary withdrawal from the market.
- This is discussed further in Chapter 1, ‘Alloplastic implantation’.
- Reported to have lower rates of capsular contracture.
Implant content
- Liquid silicone gel
- Cohesive silicone gel
- Saline
- Hydrogel
- Triglyceride
- Hyaluronic acid
- Only implants filled with silicone (semi-liquid or cohesive) or saline are available in the United Kingdom.
Shape
- Round
- Anatomically shaped
- Designed to resemble the natural breast contour.
- Less upper pole projection; more lower pole projection.
- Anatomical implants have various projections, heights and widths.
- This allows selection of an implant for a specific breast shape.
- Particularly suitable for thin patients at risk of excessive upper pole fullness.
- Designed to resemble the natural breast contour.
- There is controversy about whether shaped or round implants produce a better result:
- Proponents of anatomical implants claim they produce better breast shape.
- Proponents of round implants argue that:
- Round implants become anatomically shaped when held upright.
- Anatomical implants may rotate within their pocket.
- Round implants become anatomically shaped when held upright.
- Proponents of anatomical implants claim they produce better breast shape.
Incisions for insertion
Inframammary incision
- Most common method of inserting breast implants.
- Advantages: good exposure; ease of pocket dissection.
- Disadvantage: visible scar.
- Advantages: good exposure; ease of pocket dissection.
Axillary incision
- Relatively inconspicuous scar.
- Pocket dissection, particularly medially and inferiorly, can be difficult.
- If this is not done adequately, implants tend to displace superiorly.
Periareolar incision
- Concealed scar.
- Nipple paraesthesia and scar tenderness may occur.
Umbilical incision
- Expansion devices are inserted via the umbilicus to create a cavity under the breast.
- Collapsible saline implants are then inserted through the umbilical incision.
- Despite numerous proponents, this approach is not widely practised.
Endoscopic insertion
- The pocket can be dissected endoscopically.
- Reduces the length of the incision.
- Useful for inflatable implants inserted via an umbilical or axillary approach.
Site of implant placement
Subglandular pocket
- Deep to breast tissue but superficial to pectoralis fascia.
Subfascial pocket
- Described by Graf (1998).
- Pocket is between pectoralis fascia above and pectoralis major below.
- May decrease visibility of implants and reduce risk of capsular contracture compared to subglandular placement.
Subpectoral pocket
- Deep to pectoralis major but superficial to pectoralis minor.
- The lower pole of the implant may lie inferior to the edge of the muscle.
Dual plane
- Described by Tebbetts; a variation of subpectoral plane augmentation.
- In addition to a subpectoral pocket, subglandular dissection extends above the inferior border of pectoralis major for a variable distance towards the superior border of the NAC.
- Allows both implant placement and soft tissue redraping, which can avoid a double-bubble deformity in certain patients with ptosis.
Submuscular pocket
- Most of the pocket lies under pectoralis major.
- Laterally it lies under serratus anterior.
- Inferiorly it lies under the fascia of rectus abdominis.
- This technique was initially advocated by Scott Spear.
- He has since changed his practice with the advent of acellular dermal matrix (ADM), which is used to ensure total implant coverage.
- Laterally it lies under serratus anterior.
Pocket fashioned with acellular dermal matrix
- ADM is becoming popular in breast surgery.
- It is used in a variety of ways in both primary and secondary augmentation:
- Within the pocket to bolster areas of thin tissue.
- To minimise visible rippling.
- To support the lower pole of the implant and maintain IMF position.
- Within the pocket to bolster areas of thin tissue.
- ADM is said to reduce incidence of capsular contracture.
- It is discussed further in ‘Breast reconstruction’ and ‘Chest wall reconstruction’
The silicone controversy
- In the early 1980s, concerns arose over whether silicone implants were responsible for:
- Some types of autoimmune disease
- Increased risk of breast cancer
- Difficulties in screening for cancer.
- Some types of autoimmune disease
- In 1992, the US Food and Drug Administration (FDA) removed all silicone gel-filled breast implants from the market.
- Following years of investigation, the FDA approved specific types of Allergan and Mentor® silicone gel-filled breast implants in 2006.
- A condition of approval is that each manufacturer conducts six studies to assess the long-term performance and safety of their devices.
- The ‘Core’ study was one such study, designed to follow women for 10 years and assess effectiveness of magnetic resonance imaging (MRI) in detecting implant rupture.
- Allergan’s Core study enrolled 715 women; Mentor’s Core study enrolled 1008.
Findings of the IRG in the United Kingdom
- An Independent Review Group (IRG) was set up in the United Kingdom to examine evidence for claims that silicone had adverse health effects.
- In 1998, the report concluded silicone breast implants are not associated with greater health risk compared to other surgical implants.
- There was no evidence of:
- Association with abnormal immune response.
- Association with typical or atypical connective tissue diseases or syndromes.
- Increased risk of connective tissue disease in children of implanted women.
- Association with abnormal immune response.
- Silicone implants are associated with a number of local complications:
- Implant rupture
- Capsule formation.
- The report recommended a national implant registry to record details of all women undergoing breast augmentation.
- Implant rupture
Findings of IMNAS in the United States
- In the United States, the Institute of Medicine of the National Academy of Science (IMNAS) released its final report in June 1999, concluding:
- No evidence that silicone implants are responsible for any major diseases.
- Women are exposed to silicone constantly in their daily lives.
- No evidence that recurrent breast cancer is more prevalent in women with implants.
- Silicone breast augmentation is not a contraindication to breastfeeding.
- Cows’ milk and infant formulas contain higher levels of silicone than breast milk from women with silicone implants.
- No evidence that silicone implants are responsible for any major diseases.
Lymphoma
- In 2008, Dutch researchers studied a group of women with a rare lymphoma.
- A case–control study found women with breast implants had a higher association with a rare anaplastic large T-cell lymphoma (ALCL) subtype than those without implants.
- The odds ratio for ALCL associated with breast prostheses was 18.2.
- Nevertheless, only 34 cases of ALCL have been reported in women with breast implants throughout the world.
- This is a fraction of the estimated 10 million women who have received breast implants worldwide, making the absolute risk of ALCL very low.
Capsule formation
- Capsules form around all implants.
- In some cases, capsules contract, causing discomfort and distortion.
- Calcification of the capsule may occur.
- Rare within 10 years of implantation, but ubiquitous after 23 years.
Aetiology
- Cause of capsular contracture is unknown; suggested factors:
- Biofilm on the implant shell.
- Biofilm: ‘a complex aggregation of microorganisms growing on a solid substrate’.
- S. epidermidis was found in 90% of capsules removed for contracture, compared to 12% of capsules removed for other reasons.
- Implants may be washed in antibiotics or povidone–iodine for this reason.
- Biofilm: ‘a complex aggregation of microorganisms growing on a solid substrate’.
- Implant location.
- Submuscular placement is said to be associated with less contracture.
- Implant size.
- Implants >350 cc have greater incidence of contracture.
- Surface covering of the implant.
- Polyurethane foam covered implants have less reported contracture.
- The Allergan Core study showed textured and smooth silicone implants have similar contracture rates.
- However, most textured implants were used in reconstruction patients, who were expected to have a higher capsular contracture rate than observed.
- Polyurethane foam covered implants have less reported contracture.
- Haematoma.
- Silicone gel bleed, causing local tissue irritation.
- Foreign body reaction.
- Genetic predisposition.
- Biofilm on the implant shell.
Classification of capsular contracture
- Baker classified capsular contracture:
- Grade I: the augmented breast feels as soft as an unoperated one.
- Grade II: minimal—implant palpable, but not visible.
- Grade III: moderate—implant easily palpable, and it (or distortion from it) is visible.
- Grade IV: severe—the breast is hard, tender, painful and cold. Distortion is often marked.
- Grade I: the augmented breast feels as soft as an unoperated one.
Incidence
- Data from the Core studies show Baker III/IV contracture rates of:
- Allergan Natrelle® implants (10 years): 18.9% for primary surgery; 28.7% for revision surgery.
- Mentor MemoryGel® (8 years): 10.9% for primary surgery; 24.1% for revision surgery.
- Allergan Natrelle® implants (10 years): 18.9% for primary surgery; 28.7% for revision surgery.
Treatment
- Patients with Baker grade III or IV contracture often seek revision surgery.
- Options include:
- Closed capsulotomy
- Squeezing the augmented breast until it ‘pops’, indicating capsule rupture.
- Not recommended due to high recurrence rate, displacement or haematoma.
- Squeezing the augmented breast until it ‘pops’, indicating capsule rupture.
- Open capsulotomy or capsulectomy
- Capsulectomy associated with lower risk of recurrence, but more complications.
- Capsulectomy decreases breast volume, which may not be desirable.
- Capsulectomy associated with lower risk of recurrence, but more complications.
- Closed capsulotomy
- Capsulectomy may be preferred over capsulotomy in these circumstances:
- If the capsule is very thickened or calcified, causing contour irregularity.
- If the implant has ruptured, particularly if it is a Poly Implant Prothèse (PIP) implant.
- If the capsule is very thickened or calcified, causing contour irregularity.
- Scott Spear advocates capsulectomy, either partial or total, with replacement of the implant in a dual plane.
Poly Implant Prothèse (PIP) silicone implants
- Manufactured by a French company of the same name.
- Widely marketed in Europe, South America and Australia.
- In 2009, French authorities found silicone gel used in the implants was industrial grade, intended for mattresses and cushions.
- This had been the case since 2001.
- Case reports also indicated the 5-year risk of implant rupture was 2–6 times higher than expected.
- Based on relatively poor data, 10-year PIP rupture rates are reportedly 15–30%.
- This is broadly comparable to Allergan (13% at 10 years) and Mentor (14% at 8 years).
- Patients with PIP ruptures are more likely to have a local tissue reaction and lymphadenopathy.
- Official tests carried out in 2010 by the UK Medicines and Healthcare products Regulatory Agency (MHRA) and its French and Australian counterparts revealed no evidence of genotoxicity or cytotoxicity associated with the industrial silicone used.
- Based on relatively poor data, 10-year PIP rupture rates are reportedly 15–30%.
Recommendations of the UK Department of Health Expert Group
- Providers of PIP implants should offer consultation and investigation to determine whether implants are intact.
- Patients whose providers are unwilling to do this should be referred to a specialist via their general practitioner (GP).
- If there is any sign of rupture, explantation should be offered.
- If the implants are intact, discussion with the patient should include:
- Risks of surgery for revision augmentation—greater than for primary augmentation.
- If the implants are not removed, there is ongoing risk of rupture.
- Risks of surgery for revision augmentation—greater than for primary augmentation.
- If the patient decides against early explantation, annual review is offered.
Joint surgical guidelines for PIP implants
- Authored by five UK surgical organisations, including the British Association of Plastic Reconstructive and Aesthetic Surgeons (BAPRAS) and British Association of Aesthetic Plastic Surgeons (BAAPS).
- Surgeons should remove or exchange implants using conventional techniques, through the original incision where possible.
- Biopsy and capsulectomy is recommended for extensive capsular thickening, inflammation or contracture.
- Biopsy or capsulectomy is not required for uncomplicated, soft capsules without evidence of silicone impregnation or local inflammation.
- When there is extreme silicone contamination, consider deferring implant replacement.
- Patients with extensive lymphadenopathy or parenchymal lumpiness should be investigated and discussed by a breast multi-disciplinary team (MDT).
- Patients should be informed of the additional risks of any planned axillary surgery.
Consequences and complications of breast augmentation surgery
- Normal post-operative sequelae of surgery:
- Swelling, hardness, discomfort, bruising, pain, altered sensation.
- Usually takes months until the final result is achieved.
- Most take a few weeks off work to recover.
- Risk of not being able to breastfeed after periareolar approach.
- Swelling, hardness, discomfort, bruising, pain, altered sensation.
- Implants have a finite lifespan; almost all require replacement at some point.
- Implants can present difficulties during routine mammography.
- Specialised ‘Eklund push-back views’ improve visualisation of breast tissue during mammography.
- Implants do not adversely affect breast cancer detection, stage at diagnosis or survival.
- Patients should be told about these specific complications:
- Specialised ‘Eklund push-back views’ improve visualisation of breast tissue during mammography.
Early
- Infection, bleeding, seroma (1–3%)
- Deep infection often requires explantation.
- Decreased nipple sensation (15%)
- Nipples can also become hypersensitive and painful—may take months to improve.
Late
- Problematic capsular contracture
- Rupture rate
- The Allergan Core study showed a rupture rate of 13% for subjects and 7.7% for implants at 10 years (primary augmentation, revision augmentation and reconstruction).
- Up to 35% of ruptures are asymptomatic.
- The Mentor Core study showed a rupture rate of 13.6% at 8 years (primary augmentation).
- The Danish MRI study showed a 15% rupture rate at 10 years.
- The Allergan Core study showed a rupture rate of 13% for subjects and 7.7% for implants at 10 years (primary augmentation, revision augmentation and reconstruction).
- Problematic scarring (5%)
- Visible creasing and folding of the implant.
Other techniques of breast augmentation
Lipofilling
- Most suitable in these circumstances:
- For augmentation by one cup size.
- For increased upper pole fullness.
- Following ‘conservative’ breast cancer surgery.
- For augmentation by one cup size.
- Advantages:
- Relatively easy to learn.
- Less scarring than implant augmentation or flap reconstruction.
- Relatively easy to learn.
- Disadvantages:
- Fat necrosis, oil cysts and microcalcification, which is visible on mammograms.
- These changes can be differentiated from cancer by experienced radiologists.
- Fat necrosis, oil cysts and microcalcification, which is visible on mammograms.
- Effects of stem cells on breast tissue are controversial.
- Long-term follow-up studies have not shown increased rates of local recurrence of cancer, but these case series are relatively small.
- Recently, technical refinements have been described that achieve significantly larger breast augmentation, more fat graft placement and higher graft survival rates.
- This involves using the Brava® device, a bra-like vacuum-based external tissue expander, that is said to enlarge the subcutaneous and periglandular tissue matrix.
- Brava may also increase the vascularity of the breast.
- After 4 weeks of expansion, lipofilling is done into this expanded, vascular breast.
- Disadvantages include wearing the Brava, which many cannot tolerate for prolonged periods of time.
- Lipofilling in this procedure requires 10–14 needle puncture sites per breast, which carries a risk of hypertrophic or keloid scarring in certain patients.
Hyaluronic acid
- Non-animal stabilised hyaluronic acid (NASHA), also known as Macrolane™, was previously authorised for breast augmentation.
- It is now known that Macrolane in the breast can make diagnosing breast cancer more difficult, particularly with mammography.
- The manufacturer (Q-Med) has since discontinued this indication for its product.
The tuberous breast
- Also known as a constricted breast.
- Characterised by:
- Deficient breast base dimension
- Tight, elevated IMF
- Elongated thin breast
- Herniation of the NAC
- Stretching of the areola
- Breast asymmetry is common.
- Deficient breast base dimension
- The Northwood index was recently proposed as a more precise way to diagnose tuberous breasts.
Classification of tuberous breast deformity
- Von Heimburg classified tuberous breast deformity:
- Type I: Hypoplasia of the lower medial quadrant.
- Type II: Hypoplasia of the lower medial and lateral quadrants with sufficient skin in the subareolar region.
- Type III: Hypoplasia of the lower medial and lateral quadrants with deficient skin in the subareolar region.
- Type IV: Severe breast constriction, minimal breast base.
- Type I: Hypoplasia of the lower medial quadrant.
Surgical correction
- The tuberous breast is a difficult problem to correct.
- Principles of correction:
- Reducing the size of the areola
- Correcting nipple herniation
- Dividing any constrictions within breast parenchyma
- Lowering and releasing the IMF
- Insertion of an implant or tissue expander.
- Reducing the size of the areola
Minimal deformity
- Usually correctable by insertion of an implant.
- Lipofilling is also useful.
More severe deformity
- Usually treated with a combination of:
- Release of constrictions within breast parenchyma
- Insertion of a prosthesis or tissue expander
- Circumareolar mastopexy
- Round-block suture to limit NAC herniation.
- Extreme cases may require importation of extra skin.
- Transposition of a medially based thoraco-epigastric flap from below the IMF has been described.
- Release of constrictions within breast parenchyma
Gynaecomastia
- Enlargement of the male breast.
- Incidence varies with age; trimodal distribution:
- Up to 90% of neonates have a degree of gynaecomastia.
- 75% of boys have evidence of gynaecomastia at puberty.
- 75% of these have resolved within 2 years.
- 7% of 17-year-old boys have significant gynaecomastia.
- 75% of these have resolved within 2 years.
- 30% of middle aged men have significant gynaecomastia.
- Up to 90% of neonates have a degree of gynaecomastia.
Aetiology
- Most cases are idiopathic.
- Causes classified by three ‘P’s:
Physiological
- Neonatal
- Puberty
- Old age
Pharmacological
- Cimetidine
- Digoxin
- Diazepam
- Spironolactone
- Oestrogens
- Cannabis
- Alcohol
- Anabolic steroids
Pathological
- Cirrhosis
- Malnutrition
- Hypogonadism
- Thyroid disease
- Testicular and pituitary tumours.
Classification of gynaecomastia
- Simon classified gynaecomastia:
- Grade 1: Small, visible breast enlargement, no skin redundancy.
- Grade 2A: Moderate breast enlargement without skin redundancy.
- Grade 2B: Moderate breast enlargement with skin redundancy.
- Grade 3: Marked breast enlargement with marked skin redundancy, i.e. pendulous female breasts.
- Grade 1: Small, visible breast enlargement, no skin redundancy.
Pre-operative assessment
History
- Duration of gynaecomastia
- Pain
- Drug use
- Symptoms suggestive of a pathological cause.
Breast examination
- Assess volume of gynaecomastia
- Amount of excess skin
- Palpation of a firm central core of breast tissue below the NAC
- Abnormal breast masses.
General examination
- Genitalia
- Liver palpation
- Thyroid examination.
Investigations
- Further investigation indicated if abnormalities revealed on history and examination.
- The GP or endocrinologist may have already done this; results should be confirmed.
- Common tests required are:
- Hormones: oestrogen, testosterone, prolactin, luteinising hormone, follicle stimulating hormone, thyroid function tests.
- Biochemistry: liver function, glucose.
- Karyotyping: may be required to confirm Klinefelter’s syndrome (47XXY).
- Imaging: ultrasound of the testes.
- Hormones: oestrogen, testosterone, prolactin, luteinising hormone, follicle stimulating hormone, thyroid function tests.
Surgical correction
- Techniques include liposuction, with or without excision.
Liposuction
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


