Only selected aspects of this huge subject can be covered here. In the first part of this chapter, the skin changes seen in particular diseases (e.g. sarcoidosis) or groups of diseases (e.g. internal malignancies) are described. The second part covers some individual skin conditions that can be associated with a wide range of internal disorders (e.g. pyoderma gangrenosum).
Obvious skin signs can be seen if a tumour invades the skin, or sends metastases to it; but there are other more subtle ways in which tumours can affect the skin. Sometimes they act physiologically, causing, for example, the acne seen with some adrenal tumours, flushing in the carcinoid syndrome, and jaundice with a bile duct carcinoma. These cast-iron associations need no further discussion here. However, the presence of some rare but important conditions should alert the clinician to the possibility of an underlying neoplasm. It should be noted that the onset of these conditions might predate diagnosis of the malignancy. In some instances their natural course closely parallels that of the associated tumour and may provide the first indication of tumour relapse.
Acanthosis nigricans is a velvety thickening and pigmentation of the major flexures. Setting aside those cases caused by obesity (Figure 21.1), the metabolic syndrome (including type 2 diabetes with insulin resistance), or by drugs such as nicotinic acid used to treat hyperlipidaemia, the chances are high that a malignant tumour is present, usually an adenocarcinoma within the abdominal cavity. Acanthosis nigricans has been reported in association with the sign of Leser–Trélat, a sudden onset of multiple seborrhoeic keratoses or sudden increase in their size and number. This sign is somewhat controversial given that multiple seborrhoeic keratoses are often found in the healthy elderly population.
Erythema gyratum repens is a shifting pattern of waves of erythema covering the skin surface and looking like the grain on wood. It may precede the onset of bronchial or oesophageal neoplasms.
Acquired hypertrichosis lanuginosa (‘malignant down’) is an excessive and widespread growth of fine lanugo hair. It is more common in women, when it is usually associated with colorectal, lung and breast malignancies.
Necrolytic migratory erythema is a figurate erythema with a moving crusted edge. When present, usually with anaemia, stomatitis, weight loss and diabetes, it signals the presence of a glucagon-secreting tumour of the pancreas.
Bazex syndrome is a psoriasiform papulosquamous eruption of the fingers and toes, ears and nose, seen with some tumours of the upper respiratory tract.
Dermatomyositis, other than in childhood (p. 131). About 20% of adult patients have an underlying malignancy. However, this may be a gross under-estimation, with some series quoting figures nearer 50%. The antibody anti-P155 may be helpful in discriminating between idiopathic and malignancy-associated cases. Onset in adulthood should always prompt a thorough search for an underlying malignancy. Pay special attention to the ovaries where tumours may lurk undetected.
Generalized pruritus. One of its many causes is an internal malignancy, usually a lymphoma (p. 320).
Superficial thrombophlebitis. The migratory type has traditionally been associated with carcinomas of the pancreas.
Acquired ichthyosis. This may result from a number of underlying diseases (p. 48. Malignancy should always be excluded, in particular Hodgkin’s lymphoma (70–80% of cases) and other haematological neoplasms.
Genetic conditions. An example is the Muir–Torre syndrome in which sebaceous adenomas are accompanied by surprisingly unaggressive visceral malignancies.
Acute febrile neutrophilic dermatosis (Sweet’s syndrome; Figure 21.2). The classic triad found in association with the red oedematous plaques consists of fever, a raised erythrocyte sedimentation rate (ESR) and a raised blood neutrophil count. Aproximately 20% of cases are associated with an underlying malignancy. The most important internal association is with myeloproliferative disorders.
Paraneoplastic pemphigus (see Chapter 9). This is similar to pemphigus vulgaris but with extensive and persistent mucosal ulceration. The blisters on the palms and soles can look like erythema multiforme. It is associated with lymphoproliferative malignancies as well as underlying carcinomas.
Others. Pachydermoperiostosis is a coarsening and thickening of the skin seen in association with severe clubbing. It can be inherited as an autosomal dominant trait or be a result of the standard causes of clubbing, which include conditions such as bronchial carcinoma.
Figure 21.1 Acanthosis nigricans – in this case caused by obesity.
The following are more common in those with diabetes than in others.
Necrobiosis lipoidica. Less than 3% of diabetics have necrobiosis, but 11–62% of patients with necrobiosis will have diabetes. Apparently non-diabetic necrobiosis patients should be screened for diabetes as some will have impaired glucose tolerance or diabetes, and some will become diabetic later. The association is with both type 1 (previously termed ‘insulin-dependent’) and type 2 (previously termed ‘non-insulin-dependent’) diabetes. The lesions appear as one or more discoloured areas on the fronts of the shins (Figure 21.3). Early plaques are violaceous, but atrophy as the inflammation goes on and are then shiny, atrophic and brown–red or slightly yellow. The underlying blood vessels are easily seen through the atrophic skin and the margin may be erythematous or violet. Minor knocks can lead to slow-healing ulcers; biopsy can do the same.
No treatment is reliably helpful. The atrophy is permanent; the best one can expect from medical treatments is halting of disease progression. The disease is caused by inflammation, yet treatment with topical steroids may add to the atrophy. There is little evidence that good control of the diabetes will help the necrobiosis. A padded dressing should help those whose legs are subjected to trauma. A strong topical corticosteroid applied to the edge of an enlarging lesion may halt its expansion. Varied responses to immunosuppression and photochemotherapy have been reported.
Granuloma annulare. The cause of granuloma annulare is not known; it now seems that there is no association between the common type and diabetes. An association applies to a few adults with extensive superficial granuloma annulare, characterized by dull red or purple macules. Clinically, the lesions of the common type of granuloma annulare often lie over the knuckles and are composed of dermal nodules fused into a rough ring shape (Figure 21.4). On the hands the lesions are skin-coloured or slightly pink; elsewhere a purple colour may be seen. Although a biopsy is seldom necessary, the histology shows a diagnostic palisading granuloma, like that of necrobiosis lipoidica. Lesions tend to go away over the course of a year or two. Stubborn ones respond to intralesional triamcinolone injections. Cosmetically disfiguring cases may warrant treatment with psoralen and ultraviolet A (PUVA) treatment.
Diabetic dermopathy. In about 50% of type I diabetic patients, multiple small (0.5–1 cm in diameter) slightly sunken brownish scars can be found on the limbs, most obviously over the shins. It is thought to be caused by vascular disease and may act as a surrogate marker of systemic complications secondary to diabetes.
Candidal infections (p. 243).
Staphylococcal infections (p. 214).
Vitiligo (p. 271).
Eruptive xanthomas (p. 318).
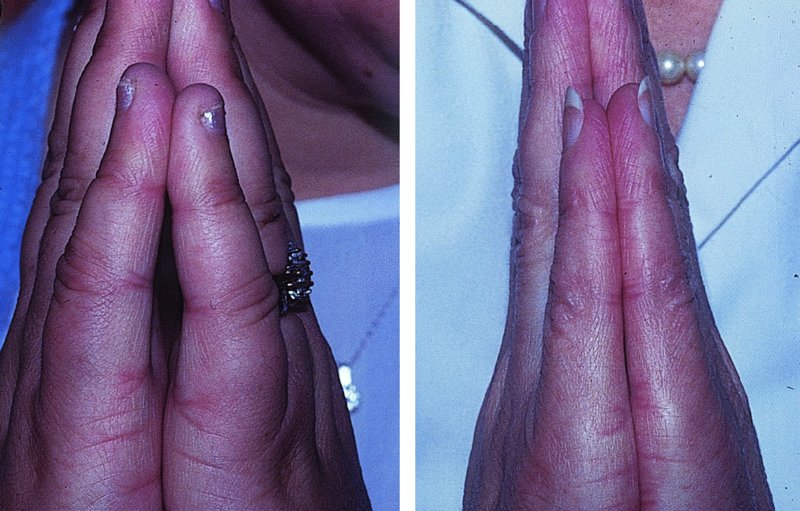
Stiff thick skin (diabetic sclerodactyly or cheiroarthropathy) on the fingers and hands, demonstrated by the ‘prayer sign’ in which the fingers and palms cannot be opposed properly (Figure 21.5).
Atherosclerosis with ischaemia or gangrene of feet.
Neuropathic foot ulcers.
Figure 21.3 Necrobiosis lipoidica: shiny yellowish patch with marked telangiectasia.
Figure 21.5 Diabetic cheiropathy – the prayer sign. Poor finger apposition in the diabetic hand (on the left) compared with the normal one (on the right).
The aetiology of sarcoidosis has yet to be fully elucidated. Current evidence suggests that in genetically susceptible individuals, an infectious or environmental antigen (as yet unknown) stimulates a predominantly Th1 immune-mediated response, resulting in the clinical manifestations discussed below. About one-third of patients with systemic sarcoidosis have skin lesions; it is also possible to have cutaneous sarcoidosis without systemic abnormalities (also known as sarcoid). The most important skin changes are as follows.
Erythema nodosum (p. 107; and Figure 8.10). This occurs in the early stages of sarcoidosis, especially in young women, and is almost always associated with hilar adenopathy. It is usually associated with transient disease and requires only symptomatic relief.
Sarcoidal granulomas in the skin. Histology reveals a ‘naked’ tubercle comprising foci of macrophages and giant cells without many surrounding lymphocytes. These are seen clinically as:
Scar sarcoidosis: granulomatous lesions arising in long-standing scars should raise suspicions of sarcoidosis.
Lupus pernio: dusky infiltrated plaques appear on the nose and fingers, often in association with sarcoidosis of the upper respiratory tract.
Papular, nodular and plaque forms (Figure 21.6): these brownish-red, violaceous or hypopigmented papules and plaques are indolent although often symptom-free. Sometimes they are annular or psoriasis-like. Lesions vary in number, size and distribution.
Figure 21.6 Sarcoidosis: plum-coloured plaques on the cheek.
Diascopy (see Chapter 3) may be helpful in the diagnosis of cutaneous sarcoid. Pressure with a glass slide over the lesion may reveal the characteristic ‘apple jelly nodules’ associated with granulomatous disease. Sarcoid is a great imitator of many conditions.
Although sarcoid may present solely in the skin it is important to assess the patient for systemic involvement as this may prompt the need for more aggressive therapy. With this in mind, a comprehensive history and examination should be performed. Investigations should include: chest radiograph; routine haematological, biochemical and bone profiles; serum angiotensin-converting enzyme (ACE) levels; urinalysis; electrocardiogram (ECG); pulmonary function tests (PFTs) and ophthalmological (slit lamp) examination. The results from these will govern the need for further investigation and referral to other specialties.
Not all cutaneous sarcoid requires treatment but for extensive disease or disease involving cosmetically sensitive areas intralesional and topical corticosteroids are sometimes helpful. If ineffective then, hydroxychloroquine, cholorquine, minocycline and methotrexate (Formulary 2, p. 426) have been used successfully. Chronic lesions respond poorly to any line of treatment short of systemic steroids, which are usually best avoided if involvement is confined to the skin. For severe disease resistant to systemic corticosteroid therapy, or when it is contraindicated, the anti-TNFα biological agents have shown significant promise.