Key points
- •
Age-associated changes throughout the face can be addressed by the judicious use of fillers.
- •
Injectable calcium hydroxylapatite (Radiesse ® ) is biocompatible, durable, non-permanent dermal filler with volumizing attributes desirable for facial contouring and rejuvenation.
- •
Applications in the upper face include brow and temporal hollow augmentation.
- •
Applications in the middle face include augmentation of the malar, submalar, and zygomatic regions, as well as nasal contouring.
- •
Applications in the lower face include correction of the nasolabial folds, oral commissure, marionette lines, and pre-jowl sulcus.
- •
Adverse events are mild, transient, and consistent with those seen with other temporary dermal fillers.
Radiesse ®
Radiesse® (Bioform Medical, San Mateo, CA) is a dermal filler approved in the United States for correction of moderate to severe facial wrinkles and folds, including the nasolabial folds (NLFs), treatment of HIV-associated facial lipoatrophy, correction of oral/maxillofacial defects, vocal fold augmentation, and as a radiographic tissue marker. This chapter describes its approved and off-label use for a variety of facial rejuvenation applications.
Radiesse® is composed of synthetic calcium hydroxylapatite (CaHA) microspheres suspended in an aqueous carrier gel in a 30% microsphere, 70% gel formulation. These uniform microspheres (25–45 microns) are smooth in shape and are identical in composition to the mineral portion of human bone and teeth. Because the components of CaHA occur naturally in the body, they are inherently biocompatible. Calcium hydroxylapatite has been used for over 20 years in various forms in surgery and dentistry. Its safety has been extensively demonstrated via in vitro and in vivo safety studies and in several retrospective clinician reports, including toxicology assessments, standardized biocompatibility testing, and a three year animal study. Radiesse® does not require patient sensitivity testing before use.
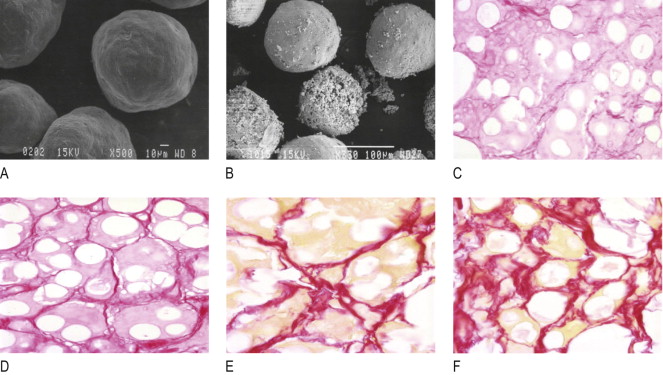
Radiesse® is injected into the dermal and subdermal planes. Upon injection, Radiesse® provides immediate correction. Over time, the carrier gel is gradually absorbed and the CaHA particles remain. The particles act as a scaffold for the formation of new tissue at the injection site, and there is evidence of new collagen formation around the microspheres ( Figure 4.1 ) ( ). When CaHA is implanted in soft tissue, collagenesis is induced ( ). The result is a highly biocompatible, long-lasting implant with similar characteristics to adjacent tissue. No calcification or osteogenesis has been reported in extensive literature describing the use of CaHA in a variety of soft tissue applications.
Radiesse® is considered a long-lasting but non-permanent filler. Over time, the CaHA particles are broken down via normal metabolic processes and eliminated through the body’s usual excretory processes. In vivo, the durability of CaHA depends on factors such as injection technique, site of material placement, and patient age and metabolism. The reported longevity of aesthetic correction in the face ranges from 10–14 months with an average correction of 1 year ( ). Other sources report longevity of correction of 12–18 months ( , ).
Patient selection
Candidates for the use of Radiesse® include patients with age-associated facial changes that are amenable to correction with dermal fillers. It has been used successfully in adult patients of various ages, genders, races and ethnicity, and with medical conditions such as human immunodeficiency virus (HIV).
Radiesse ® for facial aging
The ability of Radiesse® to provide immediate and durable effects has fueled interest in its use for expanded aesthetic applications. This is especially true in the mid- and lower face, where its volumizing properties make it particularly well suited for correcting volume loss and for aesthetic facial contouring. Potential mid- and lower face applications for Radiesse® are illustrated in Figure 4.2 .

In the remainder of this chapter, general measures for enhancing patient comfort, anticipating and minimizing potential complications, and optimizing aesthetic results are discussed, followed by recommendations for CaHA use in each area. These recommendations include anesthesia, injection techniques, and volumes for injection. The use of Radiesse® for HIV-associated facial lipoatrophy is also briefly discussed.
Operative technique
Pre-operative preparation
For any aesthetic procedure, it is important to carefully discuss expectations with each patient when planning treatment. An assiduous review of the patient’s medical history is also essential, with special emphasis on the patient’s use of prescription and non prescription medications, allergies, history of cold sores, presence of auto immune disorders, previous facial surgeries or dermal filler treatments, and whether the patient is pregnant or nursing. If the patient has a history of facial herpesvirus lesion, prophylactic antiviral therapy, e.g., aciclovir or valaciclovir, may be prescribed. For those with active lesions, treatment may be delayed.
Other topics that should be addressed with the patient include what to expect in terms of any discomfort that may occur during or after injection and possible adverse events, as well as the results that he or she can expect immediately after treatment and the likely durability of these results. Informed consent should be obtained. I advise patients to avoid any medications or supplements that might increase bleeding, e.g., salicylate drugs, nonsteroidal anti-inflammatory drugs, high doses of vitamin E, and certain herbs. There are also anecdotal reports of the use of Arnica montana , bromelain, and 1% vitamin K 1 (phytonadione) cream as prophylaxis against bruising.
Before beginning the actual procedure, a washable marker or other non-permanent tool should be used to identify the injection site. Marking is best performed with the patient sitting upright, to take into account the effect of gravity on the facial contours. Pre-treatment photographs may be taken before and after the marking. A typical tray set-up for injection of CaHA is listed in Table 4.1 .
| Anesthetic syringe: 1% lidocaine or lidocaine with epinephrine (1 : 100,000) and sodium bicarbonate |
| Syringes: 1.3 mL and/or 0.3 mL syringes of Radiesse ® , depending on initial injection or touch up |
| Needle gauge: 27-gauge, 1.25-inch |
| 4 × 4 gauze pads |
| Non-sterile gloves |
Anesthesia and other patient comfort measures
Appropriate use of anesthetics may enhance patient comfort during the injection of CaHA and other fillers. The choice of anesthesia technique depends largely on clinician and patient preference, as well as the site being treated. Options include infiltration anesthesia, nerve block anesthesia, topical anesthesia, the infiltration of tiny amounts of local anesthetic directly into the area, or some combination of these. I recommend marking the treatment site before anesthetic is administered, as infiltration may distort the skin surface and regional nerve block may have a blunting or effacing effect on creases and folds.
Local infiltration
Depending on the area to be filled, minimal amounts of lidocaine 1% and/or lidocaine with epinephrine (1 : 100,000) may be infiltrated subcutaneously.
Nerve block
Nerve blocks have the advantage of producing complete anesthesia while causing minimal alterations in superficial contours. Blockade of the infraorbital nerve can produce anesthesia extending from the area of the lower lid, through the cheeks, and the upper lip. This branch of the trigeminal nerve exits the maxilla through the infraorbital foramen. It can usually be found approximately 1 cm inferior to the orbital rim at the mid pupillary line. Infraorbital nerve blocks can be performed via direct transcutaneous infiltration of anesthetic agent or via intraoral injection up to three to four hours, depending on the type of anesthetic agent used. If the intraoral technique is used, patient comfort can be enhanced by applying topical anesthetic to the oral mucosa before injection.
The lower lip and chin area is innervated by the mental branch of the trigeminal nerve. The mental nerve may be blocked intraorally, in a similar fashion to the infraorbital nerve, when these areas are being treated. Nerve blocks in either location create profound anesthesia within minutes of injection and may last between three and four hours. In addition, some clinicians elect to use facial cooling systems in lieu of blocks, e.g., the Zimmer chiller or the Aqueduct facemask. Topical anesthesia and ice packs may also be used.
A technique for combining Radiesse® with anesthetic prior to administration has also been described in the literature ( ) but this has not been approved by the FDA. In this technique, a Luer-Lok connector is used to join a syringe containing 0.15 mL of 2% Xylocaine with a syringe containing Radiesse®. First, the plunger is depressed to introduce Radiesse® into the anesthetic. Then the Radiesse®-anesthetic mixture is pushed back and forth until it achieves homogeneity ( ). The resulting mixture enables the operator to provide anesthesia simultaneously with correction, with lowered extrusion force. It may be particularly well suited for filling relatively large areas, though anecdotal use of lower volumes has been reported as well. A topical anesthetic may be used at the site prior to the injection of the Radiesse®–anesthetic mixture.
Injection technique
Injection technique and injection volumes for Radiesse® tend to be site dependent. Because of the relative viscosity of CaHA, a 27-gauge, ![]() -inch or
-inch or ![]() -inch needle is recommended. Some physicians have reported use of a 28-gauge needle with a 27-gauge bore. (If lidocaine has been mixed with the Radiesse®, a 30-gauge needle can be used. If clogging occurs, simply change needles.) CaHA is usually injected at the subdermal plane, especially when being used to fill creases, wrinkles, and deep lines. It can be injected in the subcutaneous space superior to the periosteum, or placed on the periosteum if the intent is to augment the facial bony skeleton. Placement of CaHA on the periosteum will not stimulate bone growth in the area.
-inch needle is recommended. Some physicians have reported use of a 28-gauge needle with a 27-gauge bore. (If lidocaine has been mixed with the Radiesse®, a 30-gauge needle can be used. If clogging occurs, simply change needles.) CaHA is usually injected at the subdermal plane, especially when being used to fill creases, wrinkles, and deep lines. It can be injected in the subcutaneous space superior to the periosteum, or placed on the periosteum if the intent is to augment the facial bony skeleton. Placement of CaHA on the periosteum will not stimulate bone growth in the area.
Depending on the area being treated, CaHA may be injected in a retrograde fashion using a linear, threading, fanning, and/or cross-hatching technique. For supraperiosteal placement a bolus or depot type of injection may be used, followed by massage or molding of material to desired effect. Injection volumes vary with the location of the treatment site, the size of the area being treated, and individual patient characteristics.
In my own experience, a lesser volume of CaHA than of hyaluronic acid and/or collagen may be required to provide the same degree of correction. Two studies in particular, published in late 2007, support the finding of smaller volumes in CaHA than in several other soft tissue fillers. Smith et al compared CaHA versus collagen for the nasolabial folds in a split-face study of CaHA versus collagen for the nasolabial folds and found that, on average, the collagen-treated sides of the face required twice the volume of material (2.35 mL) to produce optimal correction as compared to the CaHA-treated side (1.22 mL) (P < 0.0001) ( ). Another study found that approximately 30% less volume of CaHA gel was required for full correction of the nasolabial folds compared to a non-animal stabilized hyaluronic acid ( ).
It may be appropriate to massage the site to ensure that no palpable lumps are present. Some clinicians routinely mold the injected area post treatment; other clinicians reserve molding for correction of undesired shapes in an effort to avoid the amplification of edema and erythema that molding sometimes creates.
Post-procedure care
Post-treatment photos should be taken as soon as the injections have been completed and the washable markings removed. Additional photos should be taken at 3, 6, 9 and 12 months post injection.
Post-treatment care involves application of ice over the injection areas to reduce and limit tissue edema and ecchymosis. Some clinicians advise patients to remain upright for the remainder of the day and sleep with the head elevated to reduce the degree of edema. Patient follow up visits are typically scheduled 2–12 weeks post-injection to document any adverse effects and, if necessary, provide further treatments to refine results.
Related posts:
 Third generation polymethylmethacrylate (PMMA) aesthetic soft tissue fillers for the correction of nasolabial folds and other applications
Third generation polymethylmethacrylate (PMMA) aesthetic soft tissue fillers for the correction of nasolabial folds and other applications
 Injectable silicone: current role
Injectable silicone: current role
 Poly -l-lactic acid (Sculptra®)
Poly -l-lactic acid (Sculptra®)
 Avoidance and treatment of complications after dermal filler injections
Avoidance and treatment of complications after dermal filler injections
 Possible causes and treatment options of dermal filler granulomas
Possible causes and treatment options of dermal filler granulomas
 Shaping the future: new outcomes in Europe
Shaping the future: new outcomes in Europe
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


