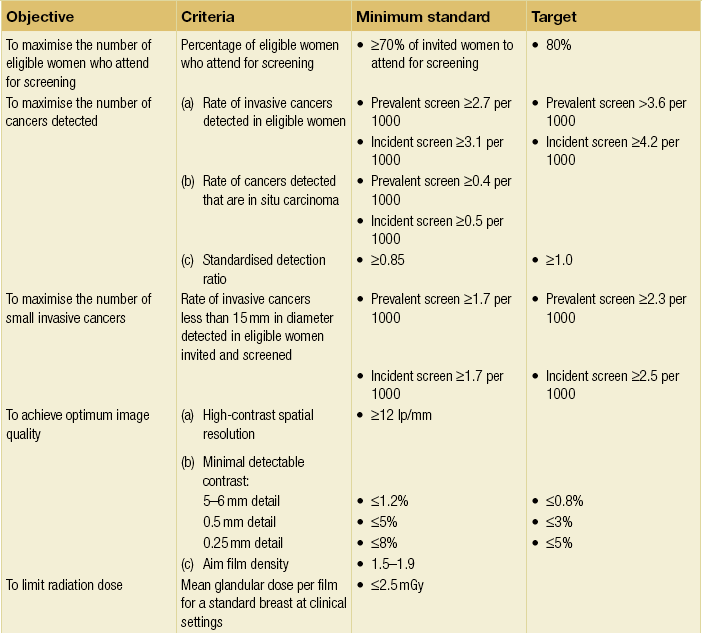
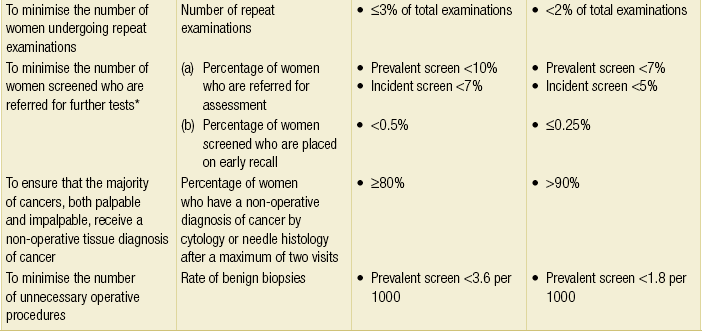
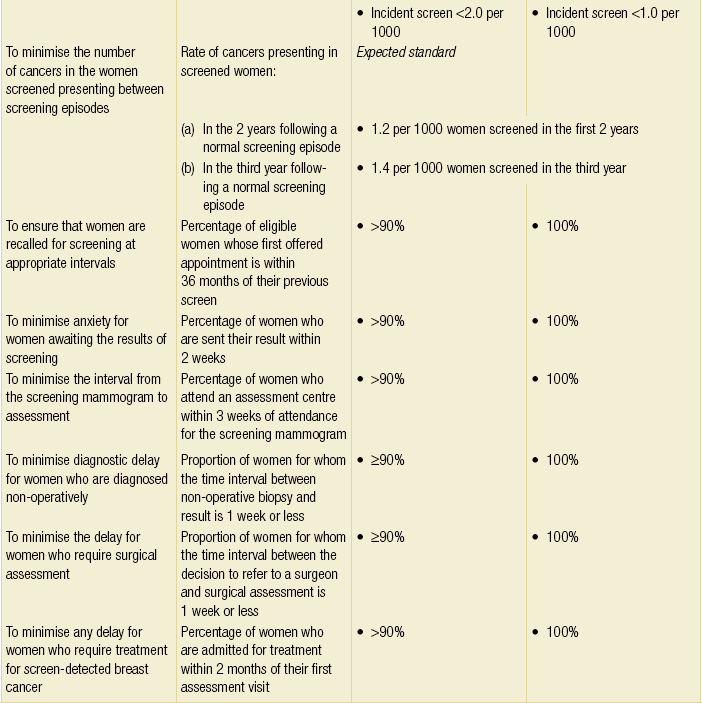
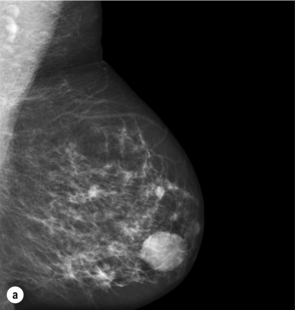
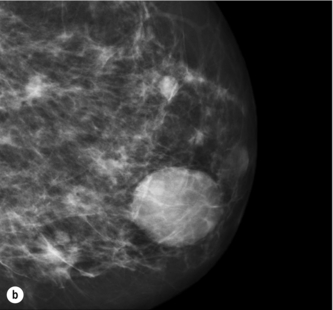
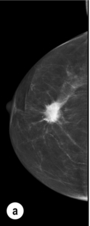
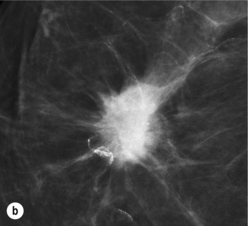
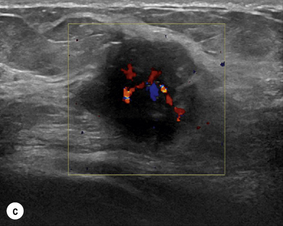
1 Breast cancer is a major health problem. Worldwide it has an increasing incidence, with over 1 million newly diagnosed cases each year, and is the commonest cancer to affect women and the commonest cause of cancer death in women. Breast cancer mortality in the UK is among the highest in the world, with approximately 28 deaths per 100 000 women per annum. This equates to around 48 000 new breast cancers diagnosed and 11 500 deaths attributable to breast cancer each year. Approximately 1 in 9 women in the UK will develop breast cancer at some time during their life.1 Early detection and improvements in treatment have led to a 30% reduction in breast cancer mortality in the UK in all age groups over the past 30 years.2 Recognising that breast cancer diagnosis and treatment required significant improvement, in 1995 the UK Department of Health published guidelines for improving outcomes in breast cancer. These guidelines were updated in 2002 and 2010 by the National Institute for Clinical Excellence (NICE).3 The guidelines emphasise the following three key issues in breast cancer care: Imaging is required at all three stages of this process, and mammography and ultrasound have a pivotal role to play. About 60% of breast cancer is diagnosed in symptomatic breast referral clinics. These clinics follow protocols that define the triple test, the combination of clinical assessment, imaging (mammography and ultrasound) and core biopsy or needle cytology, as the required standard.4 ‘One-stop’ clinics are recommended at which all the necessary tests required to make a diagnosis, including needle biopsy, are performed at one clinic visit. In order to achieve the earliest possible diagnosis of symptomatic breast cancer, women are encouraged through a variety of health promotion methods to present to these clinics as soon as they develop any change in their breasts. The clinical and imaging assessments in these clinics should be performed by appropriately trained and experienced staff. All such staff do not need to be doctors but they need to be able to give an independent opinion and be trained to an appropriate level. X-ray mammography has been the basis of breast imaging for more than 30 years. The sensitivity of mammography for breast cancer is age dependent. The denser the breast, the less effective this method is for detecting early signs of breast cancer. Breast density tends to be higher in younger women and increased density obscures early signs of breast cancer. The sensitivity of mammography for breast cancer in women over 60 years of age approaches 95%, while mammography can be expected to detect less than 50% of breast cancers in women under 40 years of age.5 Most mammography in the UK is now carried out using digital image acquisition.6–9 There are major benefits from acquiring mammograms in direct digital format.9 Compared with conventional film/screen mammography, the benefits of full-field digital mammography include better imaging of the dense breast, the application of computer-aided detection and a number of logistical advantages providing potential for more efficient mammography services.10,11 The much wider dynamic range of digital mammography means that visualisation of the entire breast density range on a single image is easily achievable. In the clinical setting, comparative studies have shown that digital mammography performs in general as well as film/screen mammography but is better in younger women and in women with dense breasts.6,7 High-frequency (≥10 MHz) ultrasound is a very effective diagnostic tool for the investigation of focal breast symptoms.12 Ultrasound does not involve ionising radiation and is a very safe imaging technique. It has a high sensitivity for breast pathology and also a very high negative predictive value.13 Ultrasound is the technique of choice for the further investigation of focal symptomatic breast problems at all ages. Under 40 years of age, when the risk of breast cancer is very low, it is usually the only imaging technique required. Over 40, when the risk of breast cancer begins to increase, it is often used in conjunction with mammography. Ultrasound is less sensitive than mammography for the early signs of breast cancer and is therefore not used for population screening. However, ultrasound does increase the detection of small breast cancers in women who have a dense background pattern on mammography.5 In the screening setting there is clear evidence that the addition of ultrasound improves small cancer detection rates, particularly in women with dense breasts, but there is currently insufficient evidence of any mortality benefit and insufficient resources to allow for routine ultrasound screening of women with dense breasts on mammography. Adding ultrasound to mammography or magnetic resonance imaging (MRI) screening does increase cancer detection but also significantly increases the false-positive rate. Ultrasound is the technique of first choice for biopsy of both palpable and impalpable breast lesions visible on scanning. Ultrasound is now used routinely to assess the axilla in women with breast cancer in most units. Axillary nodes that show abnormal morphology can be sampled accurately by fine-needle aspiration (FNA) or needle core biopsy.16,17 Discussion of the role of axillary ultrasound and FNA and core biopsy can be found in Chapter 7. Up to 50% of patients with axillary metastatic disease can be diagnosed by ultrasound combined with FNA or core biopsy, which may avoid the need for sentinel node biopsy in some women with pathologically proven nodal involvement.14,15 MRM is now widely available. In order to image the breast the patient is scanned prone and injection of intravenous contrast is required. MRM is the most sensitive technique for detection of breast cancer, approaching 100% for invasive cancer and up to 92% for ductal carcinoma in situ (DCIS), but it has a high false-positive rate.18,19,20 Rapid acquisition of images facilitates assessment of signal enhancement curves that can be helpful in distinguishing benign from malignant disease. Significant overlap in the enhancement patterns is seen, so needle sampling of the lesions detected is often required. Magnetic resonance-guided breast biopsy is available in a few centres but most breast lesions seen on MRM that are larger than 5 mm can be seen on ultrasound if they are clinically significant. MRM is the best method for screening younger women (under 40 years) at increased risk of breast cancer but, because of cost, it is unlikely to be used for general population screening.21–24 The validity of these trials was questioned in 2000–2002 but subsequent reviews by the Swedish combined trials group and a World Health Organisation International Agency for Research on Cancer committee of experts have reaffirmed the mortality benefit of mammographic screening and determined that criticisms of the mammographic screening trials were unjustified.25–30 The mortality benefit of screening is greatest in women aged 55–70 years.27,28 The mortality benefit of screening women aged between 40 and 55 is approximately 20%. Screening women under the age of 40 has not been shown to provide any mortality benefit.27,28 Breast screening has been introduced in many countries over the past 25 years. In most countries, screening is recommended in all women aged 40 and over but in countries that provide population-based screening, women of 50 and over are specifically targeted. Breast cancer screening was introduced in the UK in 1987 and provides screening by invitation, free at the point of delivery, to all women between the ages of 50 and 70.1 Women over 70 can attend but are not invited. Over 70% of the invited population need to attend for a significant overall mortality benefit to be achieved. Women under the age of 50 are not offered screening in the UK unless they are at increased risk. A randomised trial of extending the screening invitation to the age range 47–73 years was started in 2010. The results of this trial will not be available until after 2020. From 2010 screening with annual MRI in addition to mammography has been offered to women at very high risk of breast cancer, including BRCA1 and BRCA2 gene carrriers. The optimum screening method is two-view mammography; clinical examination of the breast and breast self-examination have not been shown to contribute to mortality reduction through early detection and so are not recommended.9,31,32 Women aged 50–70 in the UK are invited for mammography every 3 years. There has been some concern that this screening interval is too long. Mammography can be expected to detect breast cancer approximately 2 years before it becomes clinically apparent. The frequency of mammographic screening is determined by the lead-time of breast cancer. Based on the average growth time of breast cancer in different ages, this means that mammographic screening should ideally be carried out yearly in women aged 40–50, every 2 years in women aged 50–60 and every 3 years thereafter. However, the UK breast screening frequency trial completed in 1995 did not show any predicted benefit for women aged 50–64 screened every year compared with those screened every 3 years.33 Screening once every 3 years can be expected to detect approximately two-thirds of all breast cancers that will arise during the 3-year screening interval. HRT increases breast density and in a proportion of women this reduces the sensitivity of mammography for breast cancer.9,32–40 Up to 25% of women taking combined oestrogen/progestogen preparations continuously show increased density on mammography. This effect is significantly less with other HRT preparations. As well as reducing sensitivity HRT also reduces the specificity of mammographic screening. HRT also increases the risk of developing breast cancer.34 Breast screening programmes should have inbuilt quality assurance; the UK NHS Breast Screening Programme is subject to comprehensive quality assessment and all 100 screening units across the country have to comply with nationally defined standard guidelines. There are national targets for screening set by a central Department of Health Advisory Committee (Table 1.1). The most important cancers detected at screening are high-grade DCIS, as most cases of this type will progress to grade 2 or 3 invasive breast cancer within the following 3 years, and grade 2 and 3 invasive breast cancers under 10 mm in diameter, as at this size these tumours are much less likely to have metastasised.41,42 The common types of mammographic abnormality and their positive predictive value for cancer are shown in Table 1.2. Well-defined masses are almost always benign and do not require recall, whereas ill-defined masses and spiculated lesions always require further assessment (Figs 1.1 and 1.2). Clustered microcalcifications account for a high proportion of recalls that result in needle biopsy. More than 20% of screen-detected breast cancer is DCIS, mostly high or intermediate grade, and most of this type of cancer is detected by the presence of clustered microcalcifications (Fig. 1.3). Invasive cancer is usually represented on mammography by either an ill-defined or spiculated mass. It is essential to detect these lesions at small size as they more commonly represent grade 2 or 3 invasive cancer. Table 1.2 Positive predictive value (PPV) for malignancy of mammographic signs Figure 1.1 (a,b) Digital mammograms showing multiple well-defined masses, the typical appearance of simple breast cysts. (c) Ultrasound image showing typical features of a simple cyst, i.e. a well-circumscribed anechoic mass with distal acoustic enhancement. Figure 1.2 (a,b) Digital mammograms showing a spiculated mass in the right breast. The appearances are typical of an invasive carcinoma. The mass contains microcalcifications and there is evidence of skin tether. (c) Doppler ultrasound image showing the typical features of an invasive carcinoma with an irregular mass containing abnormal central vessels.
The role of imaging in breast diagnosis including screening and excision of impalpable lesions
Introduction
Imaging in symptomatic breast practice

Breast imaging techniques
Ultrasound

Magnetic resonance mammography (MRM)

Breast cancer screening

Population screening
Method and frequency

Factors affecting the effectiveness of screening
Quality assurance
The screening process

Sign
PPV (%)
Well-defined mass
<1
Ill-defined mass
35–50
Spiculated mass
50–90
Architectural distortion
20–40
Asymmetric density
<2
Clustered microcalcifications
15

Related posts:
 Psychosocial issues in breast cancer
Psychosocial issues in breast cancer
 Nipple discharge and the role of ductoscopy in breast diseases
Nipple discharge and the role of ductoscopy in breast diseases
 Techniques of mastectomy: tips and pitfalls
Techniques of mastectomy: tips and pitfalls
![]() The role of adjuvant systemic therapy in patients with operable breast cancer
The role of adjuvant systemic therapy in patients with operable breast cancer
![]() The genetics of breast cancer, risk-reducing surgery and prevention
The genetics of breast cancer, risk-reducing surgery and prevention
![]() Oncoplastic procedures to allow breast conservation and a satisfactory cosmetic outcome
Oncoplastic procedures to allow breast conservation and a satisfactory cosmetic outcome
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


The role of imaging in breast diagnosis including screening and excision of impalpable lesions