The Medial Plantar Flap
Arash Momeni
Subhro K. Sen
DEFINITION
The medial plantar flap is harvested from the non-weightbearing instep area of the foot.
In the majority of cases, the donor site must be skin grafted. Narrow flaps up to 2 cm in width may be closed primarily.
ANATOMY
The medial plantar flap is centered on an axis extending from the medial aspect of the first metatarsal head distally to the medial horizontal calcaneal eminence (talar shelf) proximally (FIG 1).
Perfusion to the flap is via perforators from the medial plantar artery and venae comitantes that course between the abductor hallucis and flexor digitorum brevis muscles (FIG 2).
Subcutaneous veins can be incorporated into the flap to augment venous drainage.
The medial plantar flap may be raised as a sensate flap by including branches of the medial plantar nerve.
It is critical to avoid including the weight-bearing regions of the foot (plantar forefoot, lateral plantar area, and heel) when harvesting this flap (FIG 3).
PATIENT HISTORY AND PHYSICAL FINDINGS
Preoperative evaluation of patients with plantar foot wounds includes a detailed history, focused physical examination, as well as assessment of the functional limitations associated with the foot defect.
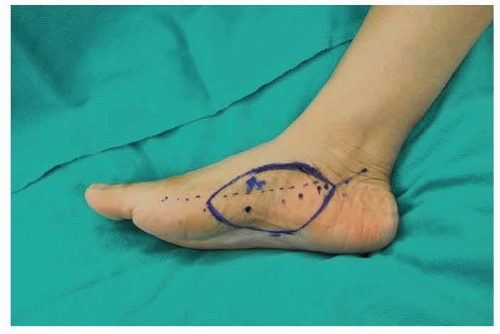
FIG 1 • Design of medial plantar flap.
History
A thorough history of pre-existing medical conditions as well as their severity must be obtained. Important conditions to identify and address preoperatively include peripheral vasculopathy, diabetes mellitus, and smoking.
Peripheral vasculopathy must be corrected prior to any attempt at reconstructing an existing ischemia-related soft tissue defect.
Diabetes mellitus management needs to be optimized to increase the likelihood of an uneventful recovery.
Preoperative smoking cessation is mandatory to decrease the risk of delayed wound healing.
A focused history of the foot wound with particular emphasis on etiology, duration, changes in size, previous wound-related complications (eg, infections), and previous attempts at treatment is critically important.
Physical examination
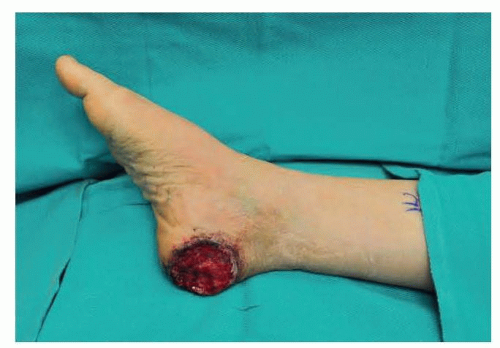
The foot wound is inspected and its location and dimensions documented.
The foot is inspected for pre-existing scars that may preclude harvest of the medial plantar flap.
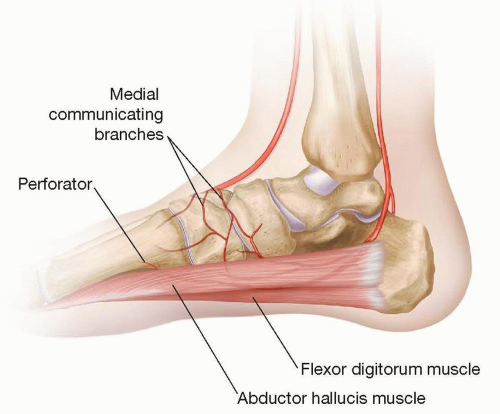
FIG 2 • Perfusion to the medial plantar flap is via perforators from the medial plantar artery and venae comitantes that course between the abductor hallucis and flexor digitorum brevis muscles.
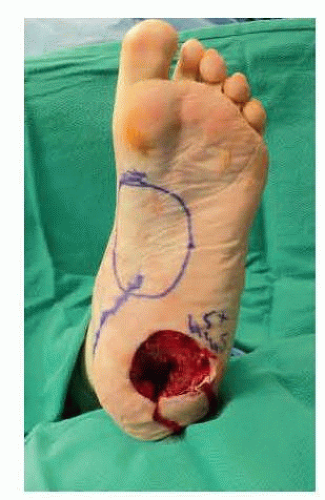
FIG 3 • Note that the medial plantar flap is designed in a manner to not include the weight-bearing regions of the foot.
A thorough neurovascular exam of the lower extremity is performed.
Pulses, that is, dorsalis pedis and posterior tibial artery, are palpated.
Doppler examination is used to confirm the presence of the medial plantar artery and identify its course.
Absence of perfusion to the foot via the dorsalis pedis artery represents a possible contraindication to utilizing the medial plantar flap, depending on arterial inflow via the peroneal artery.
Sensory examination using Semmes-Weinstein mono-filaments is performed in the distribution of the tibial as well as deep and superficial peroneal nerves.
The foot is evaluated for any acquired or congenital deformities, as these could influence the weight-bearing areas of the foot, thus, affecting flap design.
IMAGING
Preoperative imaging is not routinely required prior to harvest of the medial plantar flap.
Traditional or CT angiography can be obtained to confirm the presence of suitable pedicle vessels for patients with peripheral vasculopathy in whom there is concern for involvement of the pedicle vessels or patients with traumatic defects with the possibility of involvement of the medial plantar artery/posterior tibial artery.
Handheld pencil Doppler examination is typically sufficient to localize the medial plantar artery as well as intermuscular perforators emanating between the abductor hallucis medially and the flexor digitorum brevis muscle laterally.
SURGICAL MANAGEMENT
Patients with defects of glabrous skin containing areas are generally considered for reconstruction with the pedicled medial plantar flap based on the principle of “replacing like with like.”
It may be transferred as a free flap for reconstruction of the contralateral foot as well as volar hand and finger defects.
It is critical to examine the foot and identify weight-bearing areas so not to include these regions in the flap. The weightbearing areas include the plantar forefoot over the metatarsophalangeal heads, lateral plantar foot, and the heel.