The L Short-Scar Mammaplasty
Armando Chiari Jr.
James C. Grotting
Introduction
Breast reduction has consistently resulted in a high degree of patient satisfaction, despite the various techniques employed. However, the extensive incisions required with standard or so-called “inverted-T” reduction patterns have led plastic surgeons to seek short-scar techniques. These involve shortening or eliminating a portion of the vertical or horizontal incision while still attaining adequate reduction with good projection, shape, and symmetry.
Although these goals have proven to be elusive in very large breasts, we have found that the “L short-scar” or Chiari reduction mammaplasty yields excellent results in properly selected patients. The guiding principle of this technique is “that which remains is much more important than that which is removed.” The surgical procedure consists of resection of skin and breast tissue from the inferior and deep central portions of the breast with preservation of the main ductal system. In almost all cases of reduction, the breast base is amputated while the third, fourth, and fifth lateral intercostal nerves are preserved.
Indications and Patient Selection
Breast hypertrophy is classified as mild (resections up to 300 g), moderate (300 to 600 g), large (600 to 900 g), and very large (900 to 1,200 g or more). The Chiari reduction is best suited for women with mild to moderate mammary hypertrophy, with a resultant L short scar. Since 1999, the vertical variant of the technique has been emphasized, but now the vertical resultant scar and the mini-L scar are used for mild hypertrophies and ptosis (Figs. 98.1 and 98.2) and especially for mastopexies with associated silicone prosthesis. Patients undergoing large resections often require a secondary revision using the same technique, depending on the grade of ptosis and elasticity of the skin. Variations of the technique may be employed to avoid such revisions (see discussion). However, very large reductions, severe ptosis (grades III to IV), and insufficient skin elasticity contribute to less-than-ideal postoperative aesthetics, and such patients should be considered for an alternative reduction technique.
Because the technique is based on what will remain and not on what will be resected, we believe that one of the most important indications is the correction of asymmetry (Figs. 98.3 to 98.5). It is much easier to conceptualize reduction in the case of asymmetric breasts if one is not concerned about comparing the amounts resected from each side.
Preoperative Markings
To the surgeon unfamiliar with the Chiari reduction, the preoperative markings will appear somewhat daunting. The following description sets them down in a stepwise fashion. Since 1999, the original (1) mathematical delineation has been used only for the amount of skin necessary for reshaping the medial portion of the breast and not for the lateral portion.
Markings are based on the chest width, the vertical meridian of the chest, and the inframammary fold, rather than on a predetermined pattern. Again, the focus is on what will remain, not on what will be resected.
With the patient standing, the midmammary and midsternal lines are marked. The chest width, defined as the distance between the axillary folds, is divided by four to yield the key measurement, X. The examiner’s hand is then placed behind and under the breast, gently supporting it, to determine point A. This is the projection of the inframammary fold onto the anterior breast skin along the midmammary line above the nipple. Point A′ is now marked 2 cm above point A along the midmammary line (Fig. 98.6). The patient is now placed supine, and all subsequent marks are made with the skin under tension (Figs. 98.6B and 98.7B).
Point C is marked at a distance X cm (average 8 cm) from the midsternal line and 1 cm above the inframammary fold (Fig. 96.6). Point B is placed X + 2 cm (average 10 cm) from the midsternal line and 8 cm above point C (Figs. 96.6B and 98.7B). For larger breasts, line BC can be up to 16 cm. Point B′ is placed at one level between point A and the nipple, determined by trial and error (Figs. 98.6 and 97.7). Opposing point B to point B′ with bidigital maneuvers (Fig. 98.7A), we show the new breast cone, which must have good projection without tension (Fig. 98.7A). Point C′ is marked 7 cm from point B′, originating line B′C′C, with the skin of the lateral portion of the breast stretched in a superior and medial direction (Fig. 98.7B). Finally, point D is placed laterally, 1.5 cm above the inframammary fold along the end of the skin fold formed when line BC and B′C′ are opposed (Fig. 98.6B). The final markings form a distorted trapezoidal shape with the line B′C′ always positioned above BC. When united, lines BC (longer) and B′C′ (shorter) form the vertical reduction scar. The arching line C′D is opposed along CD to form the lateral horizontal limb (Figs. 98.6 to 98.8).
Surgical Technique
The periareolar skin bounded by points A, B, and B′ and by a vertical line extending inferiorly from B′ and by a horizontal line at the level of B is now deepithelialized. The line CD (Fig. 98.6B) is incised, and the breast tissue is dissected superiorly in the direction of the pectoralis major muscle, nearly 1 cm above the inferior border of this muscle. The breast is then extensively undermined at the level just above the pectoralis fascia, from the inferior margin of the pectoralis major to the superior breast border. Laterally, the dissection continues to the third, fourth, and fifth intercostal nerves and medially to the level of the anterior cutaneous branches of the same intercostal nerves.
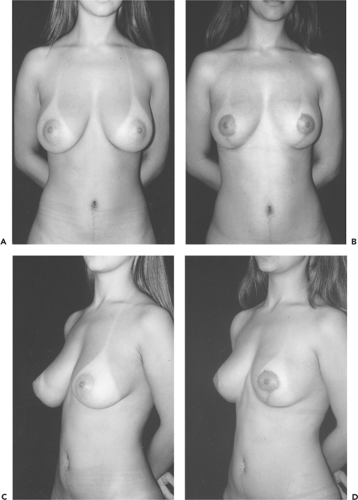 Figure 98.1. A 20-year-old patient before (A, C) and 1 year after (B, D) resection of 155 g from the left breast and 180 g from the right breast, with a “mini-L” resultant scar. |
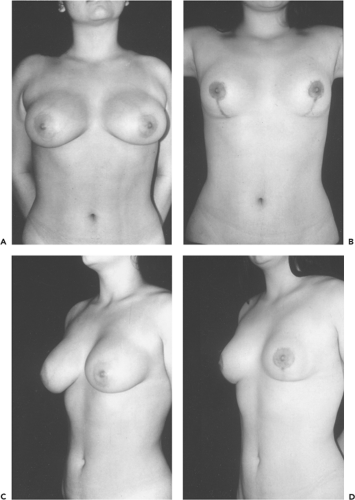 Figure 98.2. An 18-year-old patient before (A, C) and 1 year after (B, D) resection of 230 g from the left breast and 200 g from the right breast, with a vertical resultant scar.
Related posts: Follow-Up After Surgery for Primary Breast Cancer: Breast-Conserving Therapy and Mastectomy Follow-Up After Surgery for Primary Breast Cancer: Breast-Conserving Therapy and Mastectomy
 Breast Implants: Materials and Manufacturing Past, Present, and Future Breast Implants: Materials and Manufacturing Past, Present, and Future
 Reconstruction of the Irradiated Breast Reconstruction of the Irradiated Breast
 Perforator Flaps in Breast Reconstruction Perforator Flaps in Breast Reconstruction
 Lipomodeling of the Reconstructed Breast Lipomodeling of the Reconstructed Breast
 The Periareolar Approach to Augmentation Mammaplasty The Periareolar Approach to Augmentation Mammaplasty
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|