8.5 The L short-scar mammaplasty
Synopsis






Evolution of the technique and patient selection
The L short-scar mammaplasty is a reduced scar technique, which seeks to maximize the utilization of the principle that what is most important is what remains, not what is removed.1
The author’s previous publications showed the variants of the L short-scar mammaplasty with very small resulting scars – vertical and mini-L scars – with simplified markings.2,3 He tried to use these variants in most of the cases, but late evaluation showed ptosis relapse and areola enlargement in the cases of larger and more ptosed breasts. At that time, the ‘L short-scar’ or Chiari reduction was best suited for women with mild (resections up to 300 g) and moderate (300–600 g) hypertrophies. This fact instigated a reversion to indicating marking with a resulting scar in the shape of an L for most of his cases. With some improvements from years of practice, this has helped enable surgeons to perform large hypertrophies operations (resections of 600–900 g) or very large (≥900–1200 g), if the breast skin elasticity is sufficient (see Fig. 8.5.6).
The author has indicated the variants of the technique, with vertical or mini-L resulting scars to patients,2,3 the results being ptosis relapse and areola enlargement for the cases of more hypertrophy and ptosis, especially the ones whose mammary content was fatter and the skin was less elastic. In these cases, there was apparent good accommodation of the skin in the operation room, but time and gravity caused a curvature of the inferior poles and areola enlargement. Routine indication of suture in periareolar pouch4 with colorless 4-0 Mononylon® minimized, but did not solve the problem. The author reverted to indicating the technique with resulting “L” scars to patients (see Figs 8.5.6–8.5.10), with a more simplified marking (see Fig. 8.5.1A) than described in the original publication.1 Today, the markings of the variants with mini-L and vertical scars2,3 are indicated, especially for mastopexies with the associated use of prosthesis.
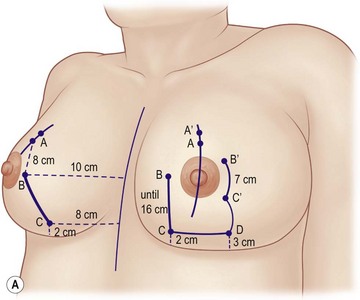
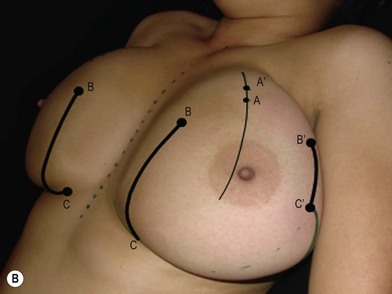


Fig. 8.5.1 (A) Point A is the projection of the inframammary fold onto the anterior surface of the breast, with the patient standing. All the other markings are made with the patient in a supine position, with the skin on stretch. The main medial markings, line BC, refer to the midsternal line, to the inframammary sulcus and to the point A. The larger and more ptosed the breast is, the longer line BC will be. (B) Markings in the operating room, in the patient of Figure 8.5.6 (resections of 1258 g and 1252 g). The larger and more ptosed the breast is, the longer line BC will be (16 cm in this patient). The larger and more ptosed the breast is, the closer point B′ should be from point A, with its lateral distance from the areola determined by trial and error: the formation of a adequate mammary cone is sought by uniting points B and B′ with bidigital maneuvers.1–3,5 (C) Same patient as in Figure 8.5.6, result in the operating room (resections of 1258 g and 1252 g). The lateral line B′C′, which was 7 cm long, was sutured to line BC, which was 16 cm long, originating the upright stem of the L scar, with some compensation folds. (D) Same patients as in Figures 8.5.1B,C and 8.5.6, result 3 months after operation. The compensation folds that result from the vertical skin compensation disappear around the third postoperative month.
One of the most important indications of this technique is asymmetry (see Fig. 8.5.9). For symmetry it is better to mark and resect directly to preserve similar portions of the breast, than to mark and resect different breast portions and only as a consequence, reach similar portions that will result in symmetry.
Since 1988, the author has performed 1287 operations using the L short-scar technique,1–3,5,6 which uses a superomedial transposition pedicle, an extensive undermining from the thoracic wall, and resects middle and inferior portions of the breast while preserving the third, fourth and fifth lateral intercostal nerves. The steps of the technique are described below.
Planning and marking
This technique’s marking is more concerned with the skin that will remain than the skin that will be removed. Markings are based on the midsternal line, the inframammary fold and its projection on the anterior surface of the breast (point A), rather than on a predetermined pattern.1 Therefore, we delimit the amount of skin strictly necessary (see Fig. 8.5.1) for reshaping the medial (line BC) and the lateral (line B′C′) portions of the breasts. After resection, the breast is reshaped by suturing together lines BC and B′C′, originating the upright stem of the L scar (see Fig. 8.5.1).
With the patient standing, the mid-mammary and midsternal lines are marked. Point A is marked on the projection of the submammary sulcus, on the mid-mammary line, and point A′ is marked 2 cm above it. Afterwards, the patient is set in dorsal decubitus and all the following marks are made on a stretched skin.1–3,5






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


