This article illustrates the author’s approach of directly excising adipose tissue excess in the lateral and posterior hip region by extending the lateral extent of the horizontal incision in a full abdominoplasty toward the posterior axillary line to produce a superior contour in this region. It is most applicable in patients with a significant adipose tissue excess in the lateral hip area that produces an outward convexity seen in the frontal, posterior, or oblique view. Such an excess represents a soft tissue “dog ear” composed of skin, and adipose tissue both deep and superficial to the superficial fascial system.
Key points
- •
This article illustrates the author’s approach of directly excising adipose tissue excess in the lateral and posterior hip region by extending the lateral extent of the horizontal incision in a full abdominoplasty toward the posterior axillary line to produce a superior contour in this region in a select group of patients.
- •
It is most applicable in patients with a significant adipose tissue excess in the lateral hip area that produces an outward convexity (a parenthesis deformity) seen in the frontal, posterior, or oblique view.
- •
Such an excess represents a soft tissue “dog ear” composed of skin, and adipose tissue both deep and superficial to the superficial fascial system or SFS.
- •
Direct excision of a various amount of skin and adipose tissue above and deep to the SFS with subsequent closure of the SFS optimizes the cosmetic appearance of the lateral hip and flank, thus creating an excellent transition between the lateral thigh and flank region while producing a modest upper thigh lift without discontinuous undermining.
- •
In the author’s experience, the contour improvements produced in this area are superior to those that result from liposuction alone in this subset of patients presenting for full abdominoplasty.
Introduction
Full abdominoplasty is the cornerstone of body contouring of the trunk and most often it includes liposuction of the lateral hips and flanks to achieve 3-dimensional contour improvement. Modern abdominoplasty techniques were developed in the 1960s, and many elements of the procedure remained largely unchanged for 3 decades. The features common to this technique have included a transverse lower abdominal incision, undermining of the abdominal skin flap often to the costal margins, tightening of the abdominal musculofascial layer by means of suture placation, and resection of the excess lower abdominal skin with inferior advancement of the abdominal flap and closure, with maximal tension at the line of skin closure occurring in the midline of the abdominal flap. Although contour improvements are realized initially in many patients, often the long-term results were suboptimal because of overtightening of the central aspect of the abdomen with accompanying superior displacement of the pubic tissues and depressed or spread scar appearance. In addition, there was often laxity of the lateral lower abdominal tissues. These shortcomings were cited by several authors, who assessed their results noted in the 1980s from a long-term perspective.
An important paradigm shift in the thinking about abdominoplasty was introduced by Lockwood, when he introduced and refined the concept of high lateral tension abdominoplasty. His insight was that the main deformity in the aging abdomen results from truncal laxity that occurred laterally in most patients and that this was not addressed by existing standard abdominoplasty approaches. To address this, he devised a procedure that entailed selective undermining of the central abdominal flap with a lesser excision of central skin and adipose excess but with a more aggressive excision of tissue in the lateral lower abdomen accompanied by a wound closure that incorporated the superficial fascial system (SFS) that achieved improved lateral contours and a more natural appearance of the central abdomen. Importantly, the selective undermining done to allow musculofascial plication preserved perforating vessels from the rectus abdominis muscles and this in turn allowed the safe application of liposuction to the upper central abdominoplasty flap. In addition, he recognized the need for circumferential contouring of the trunk to achieve true 3-dimensional esthetic contour improvement. The incorporation of liposuction of the abdominal flap and posterior trunk was the essential element of the procedure. By the late 1990s, these concepts were quickly recognized as valid by plastic surgeons around the world and have been widely adopted. In addition, they gave rise to even more aggressive approaches to body contouring in the form of body lift procedures.
The author has employed this approach for almost 2 decades but has noted that even with the high lateral tension (HLT) design the lateral wound closure frequently resulted in some element of lateral tissue excess or a “lateral soft tissue dog ear.” Very frequently this dog ear must be excised at the end of the procedure by extending the incision posteriorly. Depending on the preoperative deformity and the selected incision plan, this additional incision extension can be somewhat lengthy and has frequently required a position adjustment from the supine to a modified oblique position at the latter stages of the procedure, which makes it especially onerous for the surgeon and the surgical team. It is precisely in this area where the transition of the posterior lateral thigh to lateral flank occurs, which is an esthetically important region. The author’s experience quickly taught him that this “dog ear” consisted more of excess subcutaneous adipose tissue than a skin component in virtually all patients and is especially true for patients with thick adipose layers in the lateral and posterior hip ( Fig. 1 ). Eventually the author came to recognize that this “soft tissue dog ear” was not as completely addressed by the liposuction of the posterior hip and flank regions (which is routinely performed in >95% of his full abdominoplasty patients) as it is by the combination of liposuction followed by direct excision.
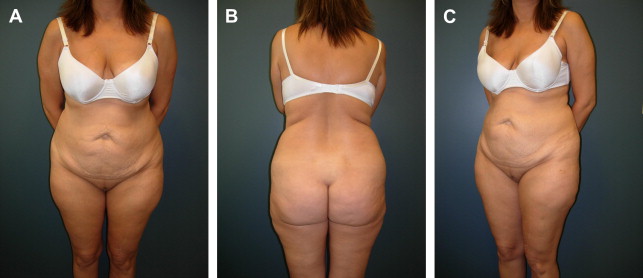
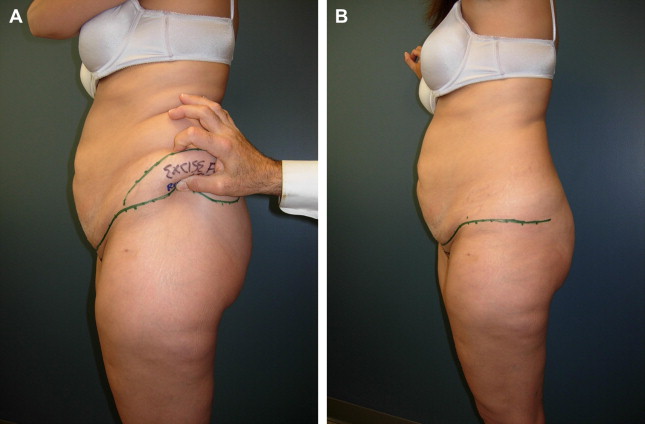
Concurrently, the author began to see and treat more patients (see Fig. 1 ) who had significant tissue excess of adipose and skin tissue in the posterior hip and flank areas that did not extend to the midline posteriorly who therefore did not require a lower body lift but rather a more aggressive approach to contour of the hip and flank regions. Because it is the author’s routine to begin almost every full abdominoplasty with liposuction of the posterior trunk with the patient in the prone position to optimize the liposuction of the back, flanks, and posterior hips, the author decided to begin the abdominoplasty in the prone position using the preoperatively placed markings ( Fig. 2 ), which were made to address the “lateral soft tissue dog ear” (see Fig. 1 A, B; Fig. 3 A), following the preliminary posterior trunk liposuction. This excision of skin and subcutaneous adipose tissue is performed down to and through the SFS. The wound closure begins medially on the posterior aspect of the trunk with apposition of the incised edges of the SFS on the posterior trunk and proceeds in a lateral direction. This SFS closure produces a modest lateral thigh lift without discontinuous undermining in the thigh area, and the contour of this area is optimized.

Preoperative evaluation
The consultation entails a detailed history focusing on the patient’s chief complaint so the surgeon can be clear about the patient’s goals and expectations relative to which areas of his or her abdominal and trunk contour are most objectionable. This history also includes recording data about the patient’s body mass index, weight stability or fluctuations, dietary, bowel, and exercise habits, waist measurement, dress size, and any history of previous abdominal surgery, types of incisions, and complications. Favorable candidates are patients who are nonsmokers, in good health, with stable weight over at least a 6-month period. A comprehensive medical history is done focusing on any history of previous venous thrombosis or other known coagulopathies, difficulty with previous anesthesia, or other significant medical problems.
Next, a careful examination of the abdomen from an esthetic standpoint is performed. The examination is carried out in both the supine and the standing positions, which enable an accurate assessment of the location and extent of skin and adipose excess and the degree of musculofascial laxity, permitting the surgeon to classify the patient’s abdominal deformity preoperatively and to select the most appropriate procedure to satisfy the patient’s goals.
Full abdominoplasty is selected in patients with significant excess of upper and lower abdominal skin and adipose tissue along with musculofascial laxity of the abdominal wall (Matarasso type IV). A detailed plan for surgery is then proposed and discussed with the patient, outlining the position and extent of incisions. As stated, it is the author’s experience that the very large majority (>95%) of patients requesting abdominoplasty will have a significant excess of adipose tissue in the posterior hip, flank, and back regions. These areas of adipose excess are most often treated with liposuction. The method of liposuction is purely the surgeon’s preference. The author strongly believes that not addressing these areas results in a significant missed opportunity to produce a balanced and harmonious 3-dimensional contour improvement in the trunk region.
Some patients present with a significant amount of adipose excess that results in a marked lateral convexity in the lateral and posterior hip region, which is immediately obvious when viewed from the anterior, posterior, or oblique vantage points (see Fig. 1 ). The author has come to think that in this subset of patients seeking 3-dimensional contour improvement liposuction alone is often not optimal. However, direct excision of this “soft tissue dog ear” performed by extending the incision posteriorly in a line similar to that used for a body lift, but not traversing the midline, addresses the problem in a more optimal way. The next section describes the technique the author uses.
Preoperative evaluation
The consultation entails a detailed history focusing on the patient’s chief complaint so the surgeon can be clear about the patient’s goals and expectations relative to which areas of his or her abdominal and trunk contour are most objectionable. This history also includes recording data about the patient’s body mass index, weight stability or fluctuations, dietary, bowel, and exercise habits, waist measurement, dress size, and any history of previous abdominal surgery, types of incisions, and complications. Favorable candidates are patients who are nonsmokers, in good health, with stable weight over at least a 6-month period. A comprehensive medical history is done focusing on any history of previous venous thrombosis or other known coagulopathies, difficulty with previous anesthesia, or other significant medical problems.
Next, a careful examination of the abdomen from an esthetic standpoint is performed. The examination is carried out in both the supine and the standing positions, which enable an accurate assessment of the location and extent of skin and adipose excess and the degree of musculofascial laxity, permitting the surgeon to classify the patient’s abdominal deformity preoperatively and to select the most appropriate procedure to satisfy the patient’s goals.
Full abdominoplasty is selected in patients with significant excess of upper and lower abdominal skin and adipose tissue along with musculofascial laxity of the abdominal wall (Matarasso type IV). A detailed plan for surgery is then proposed and discussed with the patient, outlining the position and extent of incisions. As stated, it is the author’s experience that the very large majority (>95%) of patients requesting abdominoplasty will have a significant excess of adipose tissue in the posterior hip, flank, and back regions. These areas of adipose excess are most often treated with liposuction. The method of liposuction is purely the surgeon’s preference. The author strongly believes that not addressing these areas results in a significant missed opportunity to produce a balanced and harmonious 3-dimensional contour improvement in the trunk region.
Some patients present with a significant amount of adipose excess that results in a marked lateral convexity in the lateral and posterior hip region, which is immediately obvious when viewed from the anterior, posterior, or oblique vantage points (see Fig. 1 ). The author has come to think that in this subset of patients seeking 3-dimensional contour improvement liposuction alone is often not optimal. However, direct excision of this “soft tissue dog ear” performed by extending the incision posteriorly in a line similar to that used for a body lift, but not traversing the midline, addresses the problem in a more optimal way. The next section describes the technique the author uses.
Related posts:



Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


