This article contrasts the ideal appearance of the female upper arm, axilla, and upper midlateral chest with the sagging and/or oversized deformity. The constellation of postbrachioplasty aesthetic deformity is introduced. These aesthetic shortcomings are best avoided, because they are difficult to correct. The L brachioplasty with liposuction is described in a recent case and applied to a variety of deformities to show the range of applicability and quality of results. The role of liposuction in arm reshaping is examined. The aesthetic advantages and low complication rate of the L brachioplasty are contrasted with other currently popular brachioplasties.
Key points
- •
The arm is shaped by muscular and adipose disposition and mass.
- •
Because the loose skin and fat predominantly sag along the laminar-related posterior border, the triceps-related contours can be obscured.
- •
The goal of plastic surgery of the arm is to approximate the ideal arm by removal and/or redistribution of tissues leaving the least conspicuous scars and as few complications and deformity as possible.
- •
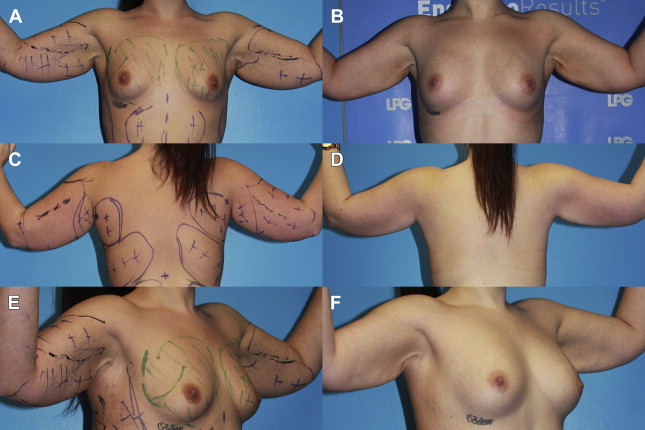
In borderline cases of excess adipose and skin, liposuction is the preferred approach, particularly in young patients after massive weight loss.
- •
When skin laxity is excessive, even in young patients, an extensive arm-long operation that extends across the axilla and onto the lateral chest is indicated.
Although the demand for brachioplasty has increased greatly over the past 10 years, there has been little attention to the aesthetics of the arm and avoidance of brachioplasty deformity. There is no consensus on technique. There also remains uncertainty as to the role of liposuction as an adjunct or alternative.
This article contrasts the ideal appearance of the female upper arm, axilla, and upper midlateral chest with the sagging and/or oversized deformity. The constellation of postbrachioplasty aesthetic deformity is introduced. These aesthetic shortcomings are best avoided, because they are difficult, if not impossible, to correct. The L brachioplasty with liposuction is briefly described in a recent case and applied to a variety of deformities to show the range of applicability and quality of results. The role of liposuction in arm reshaping is examined. The aesthetic advantages and low complication rate of the L brachioplasty, when precisely performed, are contrasted with other currently popular brachioplasties.
Women’s upper arms are tapering undulating cones extending from shoulders to elbows. A recent 1-year postoperative L brachioplasty result in a thin and muscular 67-year-old woman shows the salient aesthetics that apply across genders ( Fig. 1 ). Her frontal, right anterior oblique, and posterior images are all taken in standardized positions of the upper arm abducted 90° from the body and flexed at right angles with the arm supine. These are also the positions that the patient is asked to take when assessing redundancy of skin and fat. The extended elbow is not used, because the skin laxity about the elbow slides to the distal arm and this should not be accounted for in the upper arm resection.
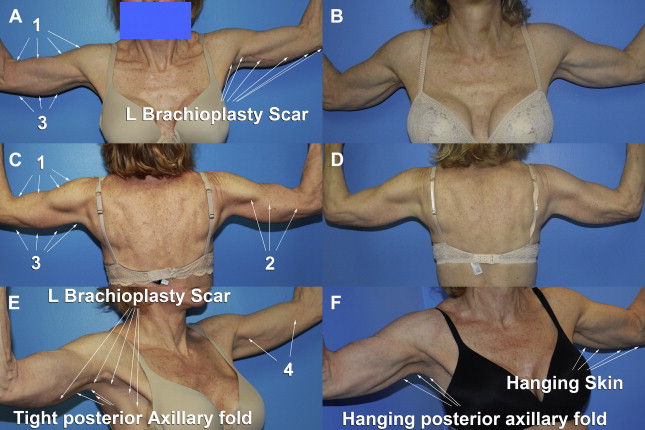
The arm is shaped by muscular and adipose disposition and mass. Description of the arm, which can be rotated into numerous positions, was standardized by Avelar in assigning the 4 sides (1) anterior, (2) external, (3) posterior, and (4) internal (see Fig. 1 ). There are 2 layers of fat. The arm is surrounded by the subdermal areolar layer of vertically segmented adipose containing the superficial neurovasculature. Only posterior is there a lamellar layer (deep) composed of horizontally oriented adipose. This deep layer is more prone to storing fat. Except for the thinnest women (as seen in Fig. 1 ), muscular definition is muted by less muscular bulk and a fuller alveolar layer. Regardless, the ideal aesthetic result in either gender is tight skin enveloping muscular curves. The deltoid and biceps muscles clearly define the bulging curves of the anterior and external arms. Separated from the biceps and brachioradialis by transverse grooves, the hanging triceps supplemented by a deposit of lamellar fat imparts a central convexity to the posterior arm. This muscle, with tightly adherent skin, acutely rises to attach to the chest to create the posterior axillary fold. The width of the most proximal arm from its attachment to the chest and the deltoid prominence is equal to the midarm from the deepest curvature of the triceps to the bulge of the biceps. The flat internal arm is accentuated by the bicipital groove, which leads to the axilla.
The axilla is a shallow dome created by the suspended clavipectoral fascia and bordered by the triceps, latissimus dorsi, and pectoralis muscles. There is a dynamic aesthetic relationship of the depth of the axilla to the position of the arm. As the arm rises from resting against the chest to full abduction and extension, the axillary recession increases to its greatest depth at 90° of abduction and progressively flattens as the arm is further raised. The central axilla is recessed by its clavipectoral fascia roof and its adherent hair-bearing skin tethered by fascia extensions through the lymph nodal area to the upper chest. Massive weight loss increases axillary depth and size.
Excess skin and fat blunt the muscle-related contours. Because the loose skin and fat predominantly sag along the laminar-related posterior border, the triceps-related contours can be obscured. Along with even more descent of the posterior axillary fold, the posterior margin evolves from curved to flat. The axillary hollow may have rolls of excess skin or deepen and widen, which is called hyperaxilla. The upper lateral chest is too full, often leading to a lateral bra roll. The definition between the lateral borders of the pectoralis major and latissimus dorsi muscles is lost.
The goal of plastic surgery of the arm is to approximate the ideal arm by removal and/or redistribution of tissues leaving the least conspicuous scars, as few complications, and as little deformity as possible. An assessment is made of the undesirable deposits of adipose and skin redundancy and laxity. Healthy youth have greater skin retraction than the aged.
In borderline cases of excess adipose and skin, liposuction is the preferred approach, particularly in young patients after massive weight loss. It is the experience of this author that preliminary focused energy results in better skin retraction to encompass the smaller volume. Radiofrequency-assisted lipoplasty of the arms has the added benefit of inducing collagen retraction through sublethal injury in borderline cases. Prolonged induration and scattered residual pockets of scarring are drawbacks. The most advanced minimally invasive bipolar technology is the BodyTite (InVasix, Israel), which remains in prolonged trials and has not yet obtained US Food and Drug Administration approval. Meanwhile, improvements in design have advanced VASERlipo to the forefront. Through 3 incisions of 4 mm, 1 in the posterior fold and 2 across the elbow, the arm is evacuated of excess superficial and deep adipose ( Fig. 2 ). Even following 54-kg (120 pound) weight loss, the resulting contours are improved with no increased laxity of skin.