There is a growing interest in upper arm aesthetic surgery but many patients do not accept the visible inner arm scar. Minimal incision brachioplasty using a shorter scar, concealed in the axilla, produces results equal to that of the traditional approach in comparable cases. Patients with massive weight loss may not meet the criteria for surgery. Patient selection and careful preoperative markings are critical to the success of the procedure. The author describes the technique he has been using for more than 30 years along with refinements. Minimal incision brachioplasty is an alternative to the traditional long scar approach in selected patients. It is a less involved procedure, with a low complication rate and high patient satisfaction.
Key points
- •
Good for many cases of brachial dermatolipodystrophy. The vertical height from the mid-humerus to the most dependent portion of the mid-upper arm (with the arm at 90° to the body) should be no greater than 12 cm. For excessive upper arm dermatolipodystrophy, the traditional method should be used.
- •
The tailor-tack method should always be used intraoperatively to confirm the accuracy of the preoperative markings. This should be done after any liposuction is performed. Corrections or modifications can be made at this time. The tailor-tack closure should always be checked with the patient in the upright position and the arm at a 90° angle to the lateral chest.
- •
A superficial plane should be used for the resection of the involved area, taking only a thin layer of fat with the resected specimen.
- •
The elbows should not be raised above the level of the shoulders until 3.5 weeks postoperatively.
- •
During preoperative marking, the transverse axis width of the incision (in the axillary fold) should stop at 1.5 to 2 cm medial to the visible portion of the axillary crease on the anterior and posterior shoulder. This helps to prevent the final scar from extending into visible areas.
- •
Undesirable anterior axillary and postaxillary fullness can also be corrected during this procedure.
- •
12% of patients need some form of revisional surgery performed at 1 year or later, most commonly for scar correction.
Introduction
The American Society for Aesthetic Plastic Surgery (ASAPS) Statistics for 2012 show that there has been a more than 800% increase in the number of brachioplasties performed in the last 15 years. Most of these patients had traditional brachioplasty, which produces predictably good results. The problem, however, is that the resulting linear scar that courses in some fashion from the axilla to the elbow can be visible when wearing sleeveless apparel. Many patients forego the operation because of the nature and visibility of the scarring.
Numerous techniques for surgical management of upper extremity contour deformities have been described since the first article published about aesthetic brachioplasty in 1954 by Correa-Iturrasspe and Fernandez. The traditional brachioplasty has stood the test of time and is still indicated for those patients with massive weight loss and excessive skin laxity.
I have been performing transaxillary brachioplasty (minimal incision brachioplasty [MIB]) for more than 30 years. In this procedure the scar is confined to the hidden area of the axilla. Inspiration for the MIB came from the seminal work of Pollack and colleagues who in 1972 introduced his revolutionary approach to the treatment of axillary hidradenitis suppurativa, which included wide excision of the involved axillary tissue with direct closure of the defect. Before this bold approach the wounds were either allowed to heal by secondary intention or skin grafted, which was followed by 3 weeks in airplane splinting.
I had the opportunity to use the Pollack technique on a large number of patients and many of the patients commented on how their arms looked aesthetically more pleasing. This unexpected feedback encouraged me to further explore the use of the Pollack technique for aesthetic improvement of the upper arm. I use the MIB on more than 95% of the patients I see with brachiodermatolipodistrophy. There have been numerous refinements in my technique for the past 30 years as I applied the technique to an ever widening spectrum of patients. Other authors have published articles on variations of this approach that are also modifications of Pollack’s original work.
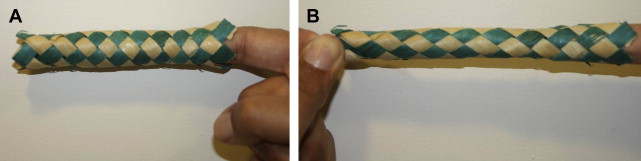
I am frequently asked how the MIB can produce such good results without the transverse excision of upper arm skin seen in the traditional brachioplasty. The answer is best demonstrated graphically using the woven bamboo finger trap ( Fig. 1 ). When one end is fixed, pulling on the opposite end causes the entire tube to narrow. Moving the skin forcibly toward the axilla produces the same effect.
Introduction
The American Society for Aesthetic Plastic Surgery (ASAPS) Statistics for 2012 show that there has been a more than 800% increase in the number of brachioplasties performed in the last 15 years. Most of these patients had traditional brachioplasty, which produces predictably good results. The problem, however, is that the resulting linear scar that courses in some fashion from the axilla to the elbow can be visible when wearing sleeveless apparel. Many patients forego the operation because of the nature and visibility of the scarring.
Numerous techniques for surgical management of upper extremity contour deformities have been described since the first article published about aesthetic brachioplasty in 1954 by Correa-Iturrasspe and Fernandez. The traditional brachioplasty has stood the test of time and is still indicated for those patients with massive weight loss and excessive skin laxity.
I have been performing transaxillary brachioplasty (minimal incision brachioplasty [MIB]) for more than 30 years. In this procedure the scar is confined to the hidden area of the axilla. Inspiration for the MIB came from the seminal work of Pollack and colleagues who in 1972 introduced his revolutionary approach to the treatment of axillary hidradenitis suppurativa, which included wide excision of the involved axillary tissue with direct closure of the defect. Before this bold approach the wounds were either allowed to heal by secondary intention or skin grafted, which was followed by 3 weeks in airplane splinting.
I had the opportunity to use the Pollack technique on a large number of patients and many of the patients commented on how their arms looked aesthetically more pleasing. This unexpected feedback encouraged me to further explore the use of the Pollack technique for aesthetic improvement of the upper arm. I use the MIB on more than 95% of the patients I see with brachiodermatolipodistrophy. There have been numerous refinements in my technique for the past 30 years as I applied the technique to an ever widening spectrum of patients. Other authors have published articles on variations of this approach that are also modifications of Pollack’s original work.
I am frequently asked how the MIB can produce such good results without the transverse excision of upper arm skin seen in the traditional brachioplasty. The answer is best demonstrated graphically using the woven bamboo finger trap ( Fig. 1 ). When one end is fixed, pulling on the opposite end causes the entire tube to narrow. Moving the skin forcibly toward the axilla produces the same effect.
Patient selection
Most of the patients I see with upper arm dermatolipodystrophy are women whose ages range from the early 40s to the mid-60s. They generally present with moderate to severe excess skin and adipose tissue of the upper arms, and feel they can no longer wear sleeveless garments. Most are not patients who have undergone massive weight loss or bariatric surgery. The MIB is applicable to most patients that I examine. For the others, the traditional approach is offered. I have used the MIB technique on several patients who exceeded the parameters for being a successful candidate. These particular patients are those who are willing to accept a lesser improvement rather than having a very visible scar on the inner arm. There is always the option of resorting secondarily to the traditional approach if they are not pleased with the outcome. I have had to do this on only two occasions.
In deciding which approach to use, I have found that if the distance as measured from the mid-humerous to the bottom of the hanging skin, with the arm at 90° to the lateral chest, is greater than 12 cm then the traditional approach should be considered. This is specifically valid if the problem is one of predominantly excess skin. Those patients, however, who demonstrate significant lipodystrophy are frequently candidates for the MIB approach because the vertical skin height is decreased by the liposuction as the skin contacts. Another exception is seen in those patients in whom vertical height is only greater than 12 cm in the upper third of the arm near the axilla, a not infrequent presentation. They do very well with the MIB approach.
A comprehensive consultation is critical to successful patient selection. Patients are shown the exact location of the axillary scar, which as is true for most body sculpture scars is visible and takes approximately 1.5 to 2 years to heal completely. This is even truer for the axillary scars, which are subjected to constant motion and friction. The terms “microscopic,” “hairline,” and “fades away” are never used. Prospective patients are also informed that about 12% to 15% of patients need some revisional surgery at 1 year. Most commonly secondary surgery is undertaken for scar revision (85% of the time) but it is also performed for removal of anterior and posterior shoulder dog ears, correction of secondary skin laxity, bow-stringing, and loss of the axillary hollow. Patients are informed that they are not allowed to raise their elbows above their shoulder level for 3.5 weeks, although movement of the forearms and some upper arm movement are permitted.
Another caution applies to those patients whose problem is predominantly crepey skin of the upper arms. This is not improved by the MIB and although the excess skin and fat are removed and good contour established, the crepey appearance remains. For these patients, the traditional brachioplasty may produce a better correction.
Finally, women who have had mastectomies and/or radiation therapy are still, if other patient selection criteria are met, candidates for the MIB. The resection is very superficial and the lymphatic system is not appreciably disturbed. I have done the MIB on several postmastectomy and postradiation therapy patients without any problems.
Surgical technique
Markings
Marking ( Fig. 2 ) is performed in the holding area with the patient in the upright position. With arms against the sides, mark the anterior and posterior shoulders at the junction between the axillary and shoulder skin. The final scar should usually not be visible beyond these markings. The entire scar should be confined to the axilla (see Fig. 2 ).
Draw a line between these two marks transversely through the apex of the axillary hollow. This line should stop 1.5 to 2 cm medial to the anterior and posterior axillary crease/shoulder junction markings. This is the first step in avoiding a final scar that extends into the visible area of the shoulder ( Fig. 3 ). Next draw a line that bisects the transverse line from the central inner arm, through the center of the transverse line to the lateral chest area (see Fig. 3 ).






