This article provides the facial plastic surgeon with anatomic and embryologic evidence to support the use of the deep-plane rhytidectomy for optimal treatment of the aging neck. An anatomic basis is established that demonstrates this technique’s ability to maximize neck rejuvenation through its direct relationship to midface soft-tissue mobilization. A detailed description of the procedure, aimed at providing safe and consistent results, is presented with insights into anatomic landmarks, technical nuances, and alternative approaches to facial variations.
Key points
- •
Neck changes are often the motivator for seeking treatment of the aging face.
- •
The platysma muscle/superficial muscular aponeurotic system/galea are the continuous superficial cervical fascia, encompassing most of the facial and neck fat. This superficial soft-tissue envelope is poorly anchored to the face and neck.
- •
Facial aging is mainly due to gravity’s long-term effects on the superficial soft-tissue envelope, with more subtle effects on the deeper structural compartments, manifesting in soft-tissue redundancy throughout the face and neck.
- •
The deep cervical fascia binds the structural aspects of the face and neck, and covers the facial nerve and buccal fat pad.
- •
The deep plane is the embryologic cleavage plane between these fascial layers and is the logical place for midfacial dissection, which allows access to the buccal fat pad for treatment of jowling.
- •
Soft-tissue mobilization is maximized in deep-plane midface dissections. Because the superficial soft-tissue envelope is continuous from the midface to the neck, this technique creates the best opportunity for reestablishing proper neck contour.
- •
Flap advancement creates tension only at the fascia level and is the optimal technique for revision rhytidectomy.
- •
The lack of skin tension in the deep-plane advancement flap allows natural, long-lasting outcomes, and is resistant to complications.
Introduction
Change in neck contour is the most common complaint that motivates a potential patient to consider a rhytidectomy. Patients desire a youthful appearance, bolstered by a well-defined neck and clear jawline. Of all facial changes associated with aging, loss of neck contour and jawline are most often associated with advanced aging.
The principal goals in neck rejuvenation, which were defined by Ellenbogen and Karlin in 1980, include creating a distinct mandibular border, subhyoid depression, thyroid bulge, a distinct border to the sternocleidomastoid muscle, and a cervicomental angle of 105° to 120°. Whereas the primary and often sole cause of blunted neck contour in younger patients is excess fat deposition, this process is not the main factor in the aging neck. Gravity’s lifetime effects on facial soft tissue, combined with facial skeletal changes and fat deposition, are the key factors that dictate neck aging. The proportions each factor contributes are based on case-specific age and anatomy.
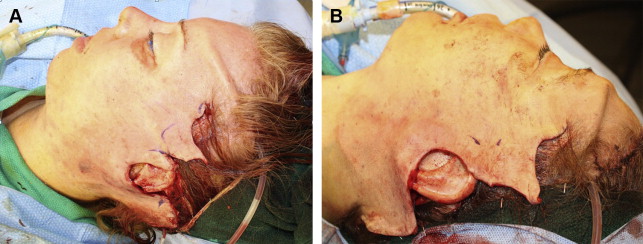
In general, gravity’s long-term downward pull on the poorly anchored facial superficial soft-tissue envelope is the central component in facial/neck aging. This process is confirmed by both facial palpation and intraoperative rhytidectomy views of the excessive, redundant facial soft tissue following sub–superficial muscular aponeurotic system (SMAS) facial dissection and flap mobilization ( Fig. 1 ). Moreover, facial skeletal remodeling causes certain aging changes, specifically around the periorbital, pyriform, and mandible regions. This process provides an explanation for the loosening of both fascial and muscular attachments, leading to pseudoherniation of fat pads and ptosis of these muscular structures. In addition, loss of mandibular height is responsible for the abrupt change in jawline and neck contour with advanced age. Fat deposition can be a contributing factor to a suboptimal neck contour at any age.
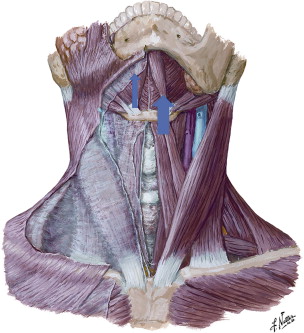
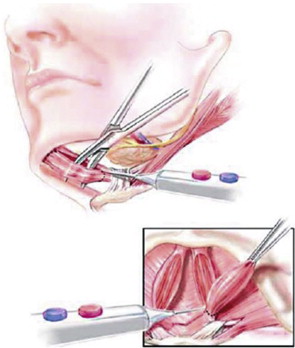
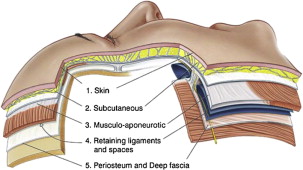
Viewing the neck in layers, most of the changes resulting from skin, fat, and muscular aging are confined to the superficial soft-tissue envelope, defined by the platysma and structures superficial to this muscle ( Fig. 2 ). Aging changes also occur in the deeper structural layers of the neck, including the subplatysmal fat, digastric muscles, and submandibular glands ( Fig. 3 ). Because these deeper neck structures can be accessed through most rhytidectomy techniques, it is the authors’ considered opinion that the most effective rhytidectomy approach to the neck is the technique that maximizes the surgeon’s ability to mobilize and resuspend the entire superficial soft-tissue envelope.
Mitz and Peyronie defined the superficial cervical facial fascia in 1976, demonstrating the SMAS to be a fibromuscular extension of the platysma muscle. Skoog advanced facelift techniques by defining the significance of the sub-SMAS dissection. Further improvement was made by Hamra in 1990 with his description of deep-plane rhytidectomy.
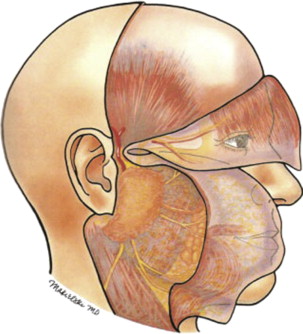
The deep plane of the face is defined as the embryologic cleavage plane separating the superficial soft-tissue envelope from the deeper structural aspects of the face, which are bounded by the deep cervical fascia ( Figs. 4 and 5 ). Dissection of the midface in the sub-SMAS/deep plane creates multiple advantages that allow for significantly improved outcomes in face and neck lifting. First, this approach enables direct deep lysis of the zygomatic cutaneous ligament, which is the major facial retaining ligament ; direct assessment and treatment of issues such as pseudoherniation of buccal fat and its influence on jowling; and mobilization of most of the facial fat. Second, because the SMAS is contiguous with the platysma muscle in the neck, sub-SMAS mobilization of the midface and superiorly/laterally based resuspension of the SMAS/platysma unit provide the best opportunity for significant and long-lasting neck rejuvenation. Third, because the deep-plane flap resuspension confines tension to the platysma/SMAS fascia, the technique is preferable for revision rhytidectomy procedures whereby avoiding or reversing skin tension is paramount to the procedure’s success. This concept further supports the deep-plane approach in treating “neck failures,” which are often due to undercorrected vertical suspension of the SMAS/platysma unit in the midface ( Fig. 6 ). Lastly, confined tension to the platysma/SMAS fascia allows for a tension-free skin closure, minimizes complications, and results in a truly natural rejuvenation.

Introduction
Change in neck contour is the most common complaint that motivates a potential patient to consider a rhytidectomy. Patients desire a youthful appearance, bolstered by a well-defined neck and clear jawline. Of all facial changes associated with aging, loss of neck contour and jawline are most often associated with advanced aging.
The principal goals in neck rejuvenation, which were defined by Ellenbogen and Karlin in 1980, include creating a distinct mandibular border, subhyoid depression, thyroid bulge, a distinct border to the sternocleidomastoid muscle, and a cervicomental angle of 105° to 120°. Whereas the primary and often sole cause of blunted neck contour in younger patients is excess fat deposition, this process is not the main factor in the aging neck. Gravity’s lifetime effects on facial soft tissue, combined with facial skeletal changes and fat deposition, are the key factors that dictate neck aging. The proportions each factor contributes are based on case-specific age and anatomy.
In general, gravity’s long-term downward pull on the poorly anchored facial superficial soft-tissue envelope is the central component in facial/neck aging. This process is confirmed by both facial palpation and intraoperative rhytidectomy views of the excessive, redundant facial soft tissue following sub–superficial muscular aponeurotic system (SMAS) facial dissection and flap mobilization ( Fig. 1 ). Moreover, facial skeletal remodeling causes certain aging changes, specifically around the periorbital, pyriform, and mandible regions. This process provides an explanation for the loosening of both fascial and muscular attachments, leading to pseudoherniation of fat pads and ptosis of these muscular structures. In addition, loss of mandibular height is responsible for the abrupt change in jawline and neck contour with advanced age. Fat deposition can be a contributing factor to a suboptimal neck contour at any age.
Viewing the neck in layers, most of the changes resulting from skin, fat, and muscular aging are confined to the superficial soft-tissue envelope, defined by the platysma and structures superficial to this muscle ( Fig. 2 ). Aging changes also occur in the deeper structural layers of the neck, including the subplatysmal fat, digastric muscles, and submandibular glands ( Fig. 3 ). Because these deeper neck structures can be accessed through most rhytidectomy techniques, it is the authors’ considered opinion that the most effective rhytidectomy approach to the neck is the technique that maximizes the surgeon’s ability to mobilize and resuspend the entire superficial soft-tissue envelope.
Mitz and Peyronie defined the superficial cervical facial fascia in 1976, demonstrating the SMAS to be a fibromuscular extension of the platysma muscle. Skoog advanced facelift techniques by defining the significance of the sub-SMAS dissection. Further improvement was made by Hamra in 1990 with his description of deep-plane rhytidectomy.
The deep plane of the face is defined as the embryologic cleavage plane separating the superficial soft-tissue envelope from the deeper structural aspects of the face, which are bounded by the deep cervical fascia ( Figs. 4 and 5 ). Dissection of the midface in the sub-SMAS/deep plane creates multiple advantages that allow for significantly improved outcomes in face and neck lifting. First, this approach enables direct deep lysis of the zygomatic cutaneous ligament, which is the major facial retaining ligament ; direct assessment and treatment of issues such as pseudoherniation of buccal fat and its influence on jowling; and mobilization of most of the facial fat. Second, because the SMAS is contiguous with the platysma muscle in the neck, sub-SMAS mobilization of the midface and superiorly/laterally based resuspension of the SMAS/platysma unit provide the best opportunity for significant and long-lasting neck rejuvenation. Third, because the deep-plane flap resuspension confines tension to the platysma/SMAS fascia, the technique is preferable for revision rhytidectomy procedures whereby avoiding or reversing skin tension is paramount to the procedure’s success. This concept further supports the deep-plane approach in treating “neck failures,” which are often due to undercorrected vertical suspension of the SMAS/platysma unit in the midface ( Fig. 6 ). Lastly, confined tension to the platysma/SMAS fascia allows for a tension-free skin closure, minimizes complications, and results in a truly natural rejuvenation.
Anatomy
By understanding the relevant facial anatomy and embryology, preference for the deep-plane rhytidectomy technique and its safe performance becomes evident. Initially viewing the layers of the face (see Fig. 5 ), one sees that the SMAS is the deep portion of the superficial soft-tissue envelope, with most facial fat distributed homogeneously superficial to this layer. This embryologic boundary is contiguous from the platysma in the neck to the galea in the forehead (see Fig. 4 ). Below this layer is the superficial layer of the deep cervical fascia, covering all the deeper embryologic structures such as the masseter muscle, facial nerve, and buccal fat pad ( Fig. 7 ). The potential space located between these layers represents the embryologic cleavage plane of the midface that defines the deep plane. Dissection in this potential space in the midface is relatively avascular, and the facial nerve is securely protected by the deep cervical fascia. In addition, the SMAS fascia fuses with the superficial layer of the deep cervical fascia at the parotid gland and is poorly defined superiorly over the facial mimetic muscles, such as the zygomatic and orbicularis muscles. Thus, most of the malar fat pad sits on this superior group of facial mimetic muscles. Crossing through these planes are the 2 facial ligaments: at the body of the zygoma are the zygomatic cutaneous ligaments (McGregor patch) and inferiorly on the medial aspect of the mandible are the mandibular ligaments, which are the sole anchors of the facial soft-tissue envelope ( Fig. 8 ).







