Jowling, submental lipoptosis, and platysmal banding can affect self-image and reduce quality of life, leading one to seek facial and neck rejuvenation. With realistic expectations, a facelift can provide the desired improvement in appearance and sense of well-being. Before any intervention, a detailed history, focused examination, communication of expected outcomes with the assistance of preoperative digital imaging, and discussion of perioperative instructions are of utmost importance. Although many techniques exist, the modified deep plane extended superficial muscular aponeurotic system rhytidectomy with submentoplasty reliably delivers a significant improvement with lasting results.
Key points
- •
The key to substantial, long-lasting improvement in rhytidectomy is to manage the neck adequately.
- •
The Kelly clamp platysmal imbrication is the foundation for an improved cervicomental angle.
- •
Skeletal augmentation and adjunctive procedures can further enhance the overall outcome.
- •
Poor incision planning with obvious scars and an altered hairline are not easily camouflaged, and are a telltale sign of rhytidectomy.
- •
Overly aggressive liposuction can lead to dermal banding and visible submandibular glands.
Introduction
Determining the patient’s aesthetic concerns is the foundation of a thoughtful discussion on rejuvenation procedures. Patients requesting a facelift may specifically request correction of facial skin laxity/ptosis and jowl formation, whereas others may primarily desire neck improvement with reduction of submental lipoptosis, relaxation of platysmal bands, and sharpening of an oblique cervicomental angle. This latter group may also appropriately ask for a facelift with different goals, or request only a necklift. They may even say, “I don’t want a facelift, all I want is a necklift.” In reality, rejuvenation of the neck and lower face are accomplished together.
The fundamental concept of rhytidectomy is based on certain anatomic relationships of the tissues. The elasticity and condition of the overlying skin, including its degree of photodamage and rhytid formation, is important. The relationship with the underlying subcutaneous tissue, including the vector of descent as a result of gravity, true ptosis, or abnormal accumulation and distribution of fat must be noted.
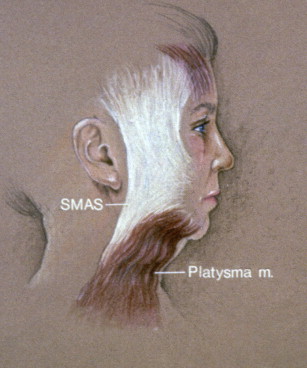
Facial musculature is enveloped by continuous fascia that extends to the preparotid region. This fascia, which is contiguous with the platysma muscle of the neck, is the superficial muscular aponeurotic system (SMAS) ( Fig. 1 ). In the neck anteriorly, the platysma muscle may or may not be interdigitated to form a connected sling depending on age. Often, there is a laxity and dehiscence of the anterior borders of the platysma muscle, creating banding in the neck. It is the very nature and the existence of this SMAS layer that allows for a deeper plane of facelifting surgery than was performed in the original rhytidectomy procedures of the past. It is easily demonstrable that lifting and pulling the SMAS layer with its integral attachment to the platysma muscle and midfacial muscles lifts and repositions the skin in the same fashion without undue tension on the skin edges. A superior and posterior vector of pull of this fascia repositions the facial and neck tissues in a more youthful position ( Fig. 2 ). The visible effect of gravity on these anatomic tissues is directly countered and improved by the facelifting procedures. It is the senior author’s practice to perform a standard platysmaplasty on all patients, in addition to the extended SMAS rhytidectomy to achieve a “sling” in the cervicomental area, which can then be used for posterior tightening of the skin–SMAS–platysma.

Treatment goals and planned outcomes
The examination begins with a general assessment of the patient’s overall health, facial features, and symmetry. Critical in analyzing patients presenting for rhytidectomy includes those items listed in Box 1 . Although all factors are important, those directly related to the neck are most critical and ultimately lead to the success of the extended SMAS rhytidectomy. Together, these factors are used to grade the patient preoperatively into one of three categories per the senior author’s classification system. A type I rhytidectomy patient demonstrates good skin elasticity, minimal jowling, minimal to no lipoptosis, early cheek and neck skin laxity, and minor platysmal laxity or banding ( Fig. 3 ). Most common is the type II rhytidectomy patient who presents with moderate facial and neck skin ptosis, clear jowling, moderate lipoptosis, and heavier platysmal banding with an obtuse cervicomental angle ( Fig. 4 ). The type III rhytidectomy patient, including most men, has heavy cheeks, prominent jowling with frequent prejowl grooves, loss of mandibular definition, significant platysmal bands with large amounts of lipoptosis, and absent cervicomental angle or convexity of the neck ( Figs. 5 and 6 ). This grading system is directly related to the expected amount of surgical work and intervention to create a long-lasting and pleasing neck contour. Additionally, the underlying skeletal structure should be noted, because a low hyoid position portends difficulty creating a sharp cervicomental angle ( Fig. 7 ). Moreover, a chin or prejowl implant can improve the structure and overall result in select cases. Lastly, the periorbital, perioral, brow, and midface should be evaluated for adjuvant procedures during rhytidectomy.
Submental and submandibular skin redundancy
Lipoptosis
Platysmal banding
Midface ptosis and hollowing
For motivated patients with realistic expectations, the extended SMAS rhytidectomy in concert with a submentoplasty is warranted. Age-related ptotic facial and neck skin, rhytids, jowl formation, platysmal banding, and lipoptosis are all indications for this surgical intervention.
Most absolute contraindications for rhytidectomy are factors that compromise wound healing of the large facial skin flap ( Box 2 ). Relative contraindications include characteristics that can lead to a less than satisfied patient. In particular, a low hyoid position limits the ability recreate an acute neckline because of the underlying suprahyoid strap muscles obstructing the placement of a high, tight platysmaplasty. A weak mandible makes enhancing the transition between the face and neck a challenge even with liposuction and tightening of the heavy overlying skin. Similarly, ptotic submandibular glands can be misinterpreted as persistent lipoptosis in the neck, and detract from a smooth lateral neck contour. If present, each of these findings should be communicated to the patient so that expectations can be managed appropriately. Some surgeons advocate partial or total excision of the submandibular glands for maximum cosmetic benefit. The senior author does not perform this procedure or believe it is an appropriate “cosmetic” indication. Lastly, a patient currently experiencing a period of high stress or a major life-changing event may be prompted to surgical intervention for the wrong reasons. This may lead to an unhappy patient when facial rejuvenation does not fulfill their goals.
Active smoking
Active vasculitidies
Active autoimmune disease of facial vasculature
Active chemotherapy or immunosuppression
Full-course facial radiation exposure
Largely fluctuating weight
Uncontrolled hypertension
Medically unfit for anesthesia
Psychologically unprepared or unfit
Unrealistic expectations
Preoperative planning and preparation
With the patient’s desires known and the examination complete, final planning begins for the extended SMAS rhytidectomy with submentoplasty. Adjuvant procedures including neurotoxins, facial fillers, skeletal augmentation, skin resurfacing, and management of the forehead, midface, and eyes are also discussed at this time. Next, digital photographs are captured to document the patient’s preoperative condition and are used as a medium for digital imaging. Standard preoperative photographic views for facelift surgery include the full-face frontal view, and full-face left and right oblique views, and left and right lateral views. One may choose a close-up perioral photograph, and a close-up showing more detail of the submental neck tissues. A close-up view of each auricle, with hair pulled behind the ears, earrings removed, and all photographs taken in a Frankfort horizontal line, is imperative. This is routinely used as a tool to further communicate a realistic representation of the expected result. Often, this is a powerful tool to demonstrate to the patient the dramatic improvement that can be expected in the neckline and jowl/jawline. A patient rarely realizes and appreciates the degree of aging changes visible from their profile. This greatly helps the patient visualize and prepare for the postoperative change. If the patient is satisfied, a date is scheduled, routine laboratory work is ordered, and the appropriate cardiac examinations and imaging are obtained. Routinely, prescriptions are given for antibiotics, analgesics, antiemetics, anxiolytics, and sleep aids at this time. Any herbals or pharmaceuticals that increase the patient’s risk of hemorrhage are discontinued in a timely manner before surgery. Finally, verbal and written instructions for the perioperative period are given to the patient.
Patient positioning
In the preoperative holding area, the markings are made with a surgical pen for the rhytidectomy and for additional procedures ( Fig. 8 ). The preauricular marking is carefully planned so as not to distort the temporal hair tuft, because it routinely stops at the inferior extent of the tuft or no higher than the upper anterior helical insertion. It incorporates a posttragal course as it is continued inferiorly in all women, and in some men. One variation in the male facelift patient with preauricular hair-bearing skin is an incision that is gently curved in the preauricular area in what is often a preexisting preauricular crease. This incision should not be entirely straight; rather, it should be a distance away from the incisura and in front of the tragus. One must leave a non–hair-bearing portion of skin when moving the bearded skin or hair-bearing skin posteriorly and superiorly ( Fig. 9 ). However, for many aging men the preauricular region bears thin or sparse hair follicles and a posttragal incision may be used. The marking then continues around the ear lobule and is placed above the postauricular sulcus on the posterior surface of the concha. As the marking reaches the level of the helical insertion, it is directed posteriorly with a gentle curve along and into the hairline. Lastly, a 3-cm marking for the submentoplasty is made in the submental crease, and the hair is twirled and taped to remove it from the operative field.





