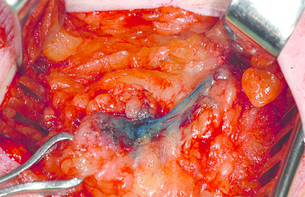
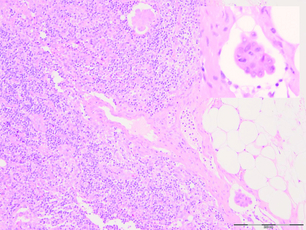
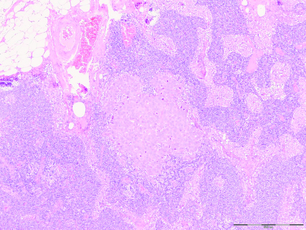
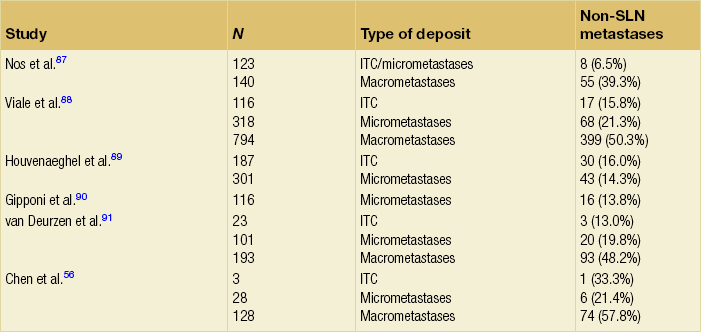
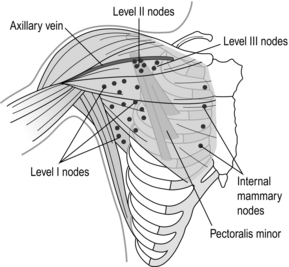
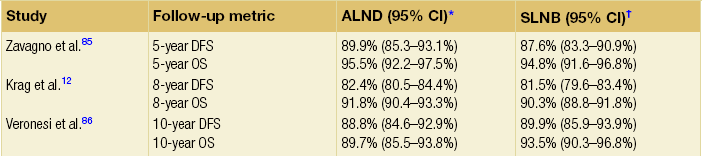
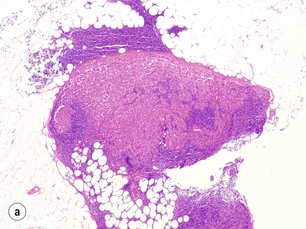
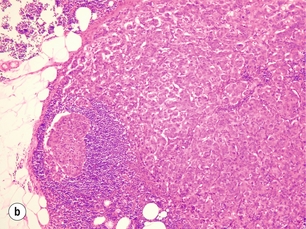
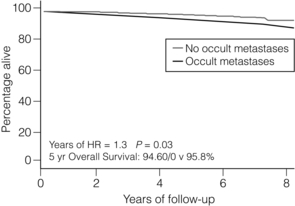
7 While there are aspects of breast surgical oncology that have moved towards a more radical approach, the management of the axilla has tended to become incrementally less invasive. Although it is clear that the status of the axillary lymph nodes continues to be the most significant prognostic marker in the management of breast cancer patients,1 removal of lymph nodes carries no survival benefit.2,3 As such, the purpose of axillary surgery in the context of breast cancer management is primarily for staging and local control. The last several decades have witnessed a metamorphosis in terms of management of the axilla, with significant paradigm shifts occurring within the last several years. Historically, a complete axillary node dissection with removal of level I and II lymph nodes or even levels I–III was standard (Fig. 7.1), and while this operation provided excellent prognostication and local control, it was associated with significant morbidity in terms of lymphoedema and decreased range of movement of the shoulder. Through the pioneering efforts of Cabanas,4 who first coined the term ‘sentinel node’ based on cadaveric studies of penile cancer, and the subsequent groundbreaking work of Donald Morton, who introduced this into the management paradigm in melanoma,5 sentinel node biopsy has revolutionised breast cancer treatment. Figure 7.1 Anatomy of the axillary nodes and levels of axillary nodes related to the pectoralis minor. Level I nodes below and lateral, level II nodes under muscle and level III nodes medial to the muscle. The concept of sentinel node biopsy is that one can map the lymphatic drainage of a tumour to the first draining lymph nodes, and that these nodes will be representative of the lymphatic basin. David Krag and Armando Giuliano6–8 introduced the technique into clinical practice for breast cancer. While initially considered an investigational procedure, large validation studies9–11 have confirmed that sentinel node biopsy is a safe, reliable, minimally invasive procedure that accurately stages the axilla. Subsequent randomised controlled trials12 have corroborated these findings (Table 7.1). The National Surgical Adjuvant Breast and Bowel Project B-32 trial found overall survival, disease-free survival and locoregional recurrence were equivalent between patients who were randomised to sentinel node biopsy followed by routine axillary dissection compared with sentinel node biopsy followed by axillary node dissection only in sentinel node-positive patients.12 Given these trial data and those from numerous other studies, sentinel node biopsy is now considered the standard of care in the management of patients with clinically node negative breast cancer. Table 7.1 Prospective randomised controlled trials validating sentinel lymph node biopsy *Sentinel node biopsy followed by routine axillary node dissection. †Sentinel node biopsy followed by axillary node dissection only in sentinel node-positive patients. Sentinel node biopsy has been validated in large cohort studies,9–11 as well as randomised controlled trials (like the NSABP B-32 trial),12 which demonstrated that the false-negative rate is low, and that survival is no different for node-negative patients who undergo sentinel node biopsy compared with axillary node dissection. Sentinel node biopsy is therefore a safe, accurate, and minimally invasive technique to stage the axilla in patients with breast cancer, and should be considered the standard of care. Considerable debate has surrounded the type of injection material used for sentinel node mapping. Some have advocated the use of blue dyes (such as patent blue V or Isosulphan blue) (Fig. 7.2) alone (severe hypersensitivity reactions with these drugs occur in approximately 1 in every 2000 patients), while others have preferred the use of radioactive tracers (such as technetium-99-labelled sulphur colloid or albumin). Still others have advocated the use of agents together. Numerous retrospective studies have found that while the false-negative rates are similar for the three techniques,7,10,13–15 identification of sentinel nodes is improved with the use of a combined technique.16 A recent prospective trial found that identification rates were 99.1% when dual tracers were used, as opposed to 93.8–95.6% for blue dye and 96.0–96.2% for radioactive tracer.17 An approach that uses radioisotope in all patients and adds blue dye only in those patients where radioisotope uptake into sentinel lymph nodes is not apparent has appeal in that it reduces the number who require blue dye. While originally many practitioners injected tracers at the site of the tumour, the concept of subareolar injection is appealing, particularly for non-palpable and/or multiple tumours, given the embryologic origins of the lymphatics in Sappey’s plexus. A number of authors have found that subareolar injection identifies the same sentinel node as a peritumoural technique,18,19 has a high identification rate, and the same false-negative rate as other techniques.17,20 Therefore, while the presence of multifocal/multicentric tumours had once been thought to be a relative contraindication to the use of sentinel node biopsy, more recent studies (many of which used a subareolar injection technique, although some utilised multiple peritumoural injections) have found the accuracy, identification and false-negative rates to be similar to smaller unifocal cancers.21 Dual tracer technique is superior to use of blue dye or radioactive tracer alone in terms of sentinel node identification and false-negative rates, and is the technique of choice to identify sentinel nodes.16,17 The subareolar injection technique has been found to be accurate in finding sentinel nodes in the setting of multifocal and multicentric breast cancer.17 Lymphoscintigraphy is often used in melanoma, where drainage patterns can vary widely; however, in breast cancer, where 98–99% of lymphatics drain to the ipsilateral axilla, (Fig. 7.3) lymphoscintigraphy has not been found to be of significant value (uptake of sentinel nodes of radioisotope takes minutes only, allowing injection of isotope after induction of anaesthesia).22,23 In cases of recurrent breast cancer, however, particularly if 10 or more lymph nodes have previously been removed, alternative drainage pathways may be encountered and lymphoscintigraphy is recommended.24 Even in patients who have had prior complete axillary node dissections, Kaur et al. have demonstrated that lymphoscintigraphy can identify drainage in 29% of patients and, of these, drainage may be non-axillary (contralateral and/or internal mammary) in 38% of cases.25 Furthermore, of the non-axillary sentinel nodes biopsied in the recurrent setting, 40% were positive and thus may alter management plans.25 Figure 7.3 Scintiscan showing drainage of technetium-99 m human albumin colloid to show multiple sentinel axillary nodes. Frozen section is the most common technique used, and is associated with a specificity of 99–100% and a sensitivity of 57–74%.26 The sensitivity is far better for macrometastases (84–92%) than micrometastases (17–61%),26 and may be particularly difficult to interpret in patients with invasive lobular carcinomas who have cytologically bland cells and an infiltrative growth pattern. Nonetheless, the overall accuracy of this technique is 83–91%.26 Tew et al. conducted a meta-analysis of 31 studies of touch imprint cytology, and found that specificity and sensitivity of this technique were 94–100% and 34–95% respectively.27 Pooled estimates from 11 studies comparing macro- and micrometastases found that the sensitivity for touch imprint cytology was significantly better for the larger deposits: 81% (95% confidence interval (CI) 74–86%) vs. 22% (95% CI 14–33%) for macro- and micrometastases, respectively.27 On a more global level, the sensitivity of touch imprint cytology is lower than that of frozen section (62% (95% CI 53–70%) vs. 76% (95% CI 65–84%)), while specificity is comparable for both (99%).27 Molecular techniques are available that detect cancer cells in sentinel nodes but these have not found widespread utility. For women at high risk who are undergoing prophylactic mastectomy, some have advocated sentinel node biopsy, as this avoids the need for subsequent axillary surgery if there is an occult breast cancer that is noted on final pathology, and the sentinel node is negative. Others, however, have argued that the risk of there being a cancer with associated lymph node metastasis is so low in the prophylactic setting that routine sentinel node biopsy, despite being of minimal additional morbidity, is not warranted. In a meta-analysis of six papers including 1251 patients who underwent 1343 prophylactic mastectomies, the rate of occult invasive cancer was 1.7% and the rate of positive sentinel nodes was 1.9%.28 Patients with positive sentinel nodes in the prophylactic setting have often been found to have had a locally advanced breast cancer in the originally treated breast so, in these patients, sentinel node biopsy may be warranted when a prophylactic contralateral mastectomy is being performed.28,29 Some have argued that patients with DCIS who are at high risk of having concomitant invasive disease should have a sentinel node biopsy at the time of their excisional surgery to obviate the need to return to the operating room for a sentinel lymph node biopsy should an invasive focus be found on final pathology. The rate of DCIS on large core biopsy being upgraded to invasive disease on final pathology is reported to be up to 47%.21,30–32 Fewer samples and the use of non-vacuum-assisted devices increase the rates of underestimation of invasive disease.32 Further, clinical factors such as young age, a palpable mass, large tumour size by imaging, high grade, and comedo necrosis are also associated with an increased risk of concomitant invasive disease in patients with core biopsy diagnosis of DCIS.33,34 While some argue that such patients should have a sentinel lymph node biopsy, others prefer to confirm diagnosis of invasive disease before subjecting patients to a potentially unnecessary lymph node evaluation procedure. While sentinel node biopsy is minimally invasive and associated with few risks, it is not innocuous. It is well established that sentinel node biopsy can be performed after breast-conserving surgery has been performed. A recent meta-analysis comparing sentinel node identification and false-negative rates for patients who underwent surgical versus needle biopsy found that rates were comparable (sentinel node identification rates 91.3% vs. 92.8%; false-negative rates 12.3% vs. 9.9%).35 Therefore, prior surgery does not affect the ability to perform this technique accurately and consensus guidelines have accepted that sentinel node biopsy should not be performed routinely in patients with DCIS undergoing breast-conserving surgery. It is accepted that for patients undergoing mastectomy for DCIS, a sentinel lymph node biopsy should be considered at the same time as the mastectomy,36,37 as this technique cannot be performed once the breast is removed and an invasive focus is identified. In those with confirmed DCIS the node positivity rate is low at < 1%. Some have argued that sentinel node biopsy should be performed prior to neoadjuvant systemic therapy. Studies have demonstrated a high identification (98–100%) and an exceedingly low false-negative rate (0%) in this situation.38 Given that this technique is performed prior to any therapy, there can be no confounding of negative results as a result of therapy, which has resulted in false-negative rates as high as 39% in selected series39 reported in patients who have a sentinel node biopsy following chemotherapy. Others, however, have argued that to do a sentinel node biopsy prior to chemotherapy eliminates the opportunity to spare the 2–35% of patients who have a pathologically complete response in the axilla the morbidity of an axillary dissection.38 Furthermore, to evaluate sentinel nodes after neoadjuvant therapy, when surgery for the primary tumour is planned, may reduce the need for a second operative procedure. A recent meta-analysis has demonstrated that sentinel node biopsy after neoadjuvant chemotherapy is associated with identification rates of between 71% and 100% (summary estimate 90.9%), false-negative rates between 0% and 39% (summary estimate 10.5%), and accuracy rates between 77% and 100% (summary estimate 94.4%).40 Two groups have performed trials of sentinel lymph node biopsy (SLNB) in the neoadjuvant setting in women with node positive breast cancer whose nodes are cleared by chemotherapy. The issue these trials addressed is whether axillary dissection (AD) can be avoided in responding patients. The ACOSOG Z1071 trial was a single arm study of 756 women (T0-4, N1-2, M0) undergoing neoadjuvant chemotherapy (NAC) with axillary nodal involvement confirmed by ultrasound guided FNA or core biopsy.41 Some patients had the involved nodes clipped. Following completion of NAC, SLNB was performed and there had to be at least 2 SLNs removed before proceeding to AD. The primary endpoint was to determine if the false negative rate (FNR) was <10% in women with N1 disease who had at least 2 sentinel nodes biopsied after NAC. Of 643 patients with a SN identified, 40.3% had a complete pathological response in the axilla. SLNB correctly identified nodal status after NAC in 84% of 695 patients. There was a 12.6% false negative rate (higher than the primary endpoint of 10%). The false negative rate (FNR) was significantly lower (10.8%) if dual tracer with both radiolabelled colloid and blue dye was used, compared with blue dye (4/24 – 16.7%) or radioisotope alone (20/101 – 20%) (p=0.046). The FNR was lower if more than 2 nodes were examined, 9.8% for 3 sentinel nodes, 6.7% for 4 sentinel nodes, but 11% for 5 or more, p=0.004 for trend. Placement of a clip in the positive node at diagnosis also decreased the FNR to 7.4% vs 13.6% without clip placement. An apparent chemotherapy effect in the SNs removed as marked by greater fibrosis or other histopathological changes in the sentinel nodes was also associated with a lower FNR (10.8% vs 13.5% without). Avoiding a high rate of false negatives in patients with node positive disease is essential and the results of this study highlight that technical factors are important for accurate SLNB after NAC. Performance can be improved by the use of dual tracer, examination of a minimum of 2 sentinel lymph nodes and placement of clips in involved nodes at diagnosis. These are the requirements if this technique is to be used after NAC. The German Breast Group addressed the issue of optimal timing for sentinel lymph node in the prospective German, multi-institutional SENTINA-trial.42 Of 1737 patients entered, 1022 women were clinically node negative and underwent SLNB prior to NAC. The SLN detection rate in this group of women was 99.1 % (1013/1022). Among these, 360 patients had histologically involved nodes and these women underwent a second SLNB followed by AD after NAC. The SLN detection rate in these patients undergoing their second SLNB after NAC was 60.8% (219/360). 592 patients, who presented initially with suspicious axillary nodes converted to a cN0 status after NAC and underwent SLNB, combined with AD. The SLN detection rate in these women was 80.1% (474/592). The difference between the detection rates of these three groups was highly statistically significant (p < 0.001). More thorough pathological evaluation of sentinel lymph nodes using serial sectioning and immunohistochemistry has allowed identification of occult metastases in up to 31% of previously ‘node-negative’ patients.43 This stage migration, and the relevance of this previously undetected disease, has been a source of considerable controversy. The American Joint Committee on Cancer classifies sentinel node metastases into three categories: ‘isolated tumour cells’ for metastases < 0.2 mm (which are considered node negative, pN0(i +); Fig. 7.4); ‘micrometastases’ for deposits between 0.2 and 2.0 mm (considered node positive, pN1mi; Fig. 7.5); and ‘macrometastases’, defined as deposits > 2.0 mm (also considered node positive, pN1a; Fig. 7.6).1 These somewhat arbitrary cut-offs have generated debate as to the true implications of both isolated tumour cells and micrometastases. Figure 7.6 Axillary lymph node with an obvious macrometastasis: (left) low power; (right) high power. In a pooled analysis of 58 studies of patients with metastases < 2 mm, de Boer et al. found that the presence of this small-volume disease in the axillary lymph node was associated with a reduction in survival, which was independent of other prognostic variables (hazard ratio (HR) = 1.44; 95% CI 1.29–1.62).44 Data from the National Surgical Adjuvant Breast and Bowel Project (NSABP) B-32 trial (Fig. 7.7) showed that any occult metastases were associated with a small increased risk of death (HR = 1.40; 95% CI 1.05–1.86), any outcome event (HR = 1.31; 95% CI 1.07–1.60) and distant disease (HR = 1.30; 95% CI 1.02–1.66).45 On subgroup analysis, isolated tumour cells had a smaller increased risk of death, any outcome event and distant disease than micrometastases. The hazard ratios (95% CI) for these three outcomes were 1.27 (1.04–1.54), 1.18 (1.02–1.33) and 1.19 (1.00–1.41), respectively, for isolated tumour cells, and 1.60 (1.32–1.96), 1.38 (1.15–1.60) and 1.41 (1.19–1.68), respectively, for micrometastases.45 The absolute differences in outcomes were, however, very small and the recommendations of the trial committee were that the differences were such that a search for occult metastases by immunohistochemistry on a routine basis when assessing sentinel lymph nodes could not be supported. The ‘Micrometastases and Isolated Tumour Cells: Relevant and Robust, Or Rubbish’ (MIRROR) Study also found that patients with both isolated tumour cells and those with micrometastases who did not receive systemic adjuvant therapy had a higher adjusted event rate than node-negative patients (HR = 1.50, 95% CI 1.15–1.94 and HR = 1.56, 95% CI 1.15–2.13, respectively).46 Figure 7.7 Data from NSABP B32 trial comparing overall survival in patients with no metastases vs occult metastases demonstrated on immunohistochemistry. A number of authors have evaluated the significance of isolated tumour cells and micrometastases in terms of the likelihood of there being other non-sentinel node metastases (Table 7.2). Cserni et al., in a meta-analysis of 25 studies, reported that up to 57% of patients with isolated tumour cells or micrometastases had non-sentinel node involvement.47 The pooled estimates for non-sentinel node involvement vary with tumour burden in the sentinel nodes, and are 20.2% (95% CI 15.5–24.9%) for micrometastases and 9.4% (95% CI 6.2–12.6%) for isolated tumour cells.47 In keeping with these data, van Deurzen et al. found that 12.3% (95% CI 9.5–15.7%) of patients with isolated tumour cells or micrometastases had non-sentinel node involvement.48
The axilla
current management including sentinel node and lymphoedema
Introduction

Sentinel lymph node biopsy: technique

Use of lymphoscintigraphy

Intraoperative evaluation
Sentinel lymph node biopsy: controversial situations
Prophylactic mastectomy
Ductal carcinoma in situ (DCIS)
Neoadjuvant chemotherapy
Isolated tumour cells and micrometastases
Non-sentinel node metastases
Related posts:
 Psychosocial issues in breast cancer
Psychosocial issues in breast cancer
 Nipple discharge and the role of ductoscopy in breast diseases
Nipple discharge and the role of ductoscopy in breast diseases
 Techniques of mastectomy: tips and pitfalls
Techniques of mastectomy: tips and pitfalls
![]() The role of adjuvant systemic therapy in patients with operable breast cancer
The role of adjuvant systemic therapy in patients with operable breast cancer
![]() The genetics of breast cancer, risk-reducing surgery and prevention
The genetics of breast cancer, risk-reducing surgery and prevention
![]() Oncoplastic procedures to allow breast conservation and a satisfactory cosmetic outcome
Oncoplastic procedures to allow breast conservation and a satisfactory cosmetic outcome
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


The axilla: current management including sentinel node and lymphoedema