Tessier’s classification system for rare craniofacial clefts remains the most widely used today. It denotes the position of the cleft process in a schema based around the orbit, and facilitates communication between surgeons regarding these complicated conditions. Tessier’s classification is reviewed in detail, and a separate discussion of hypertelorism (increased distance between the bony orbits) follows, focusing on orbital hypertelorism in the setting of craniofacial clefts.
Key points
- •
Tessier’s classification of craniofacial clefts denotes their position on the skull and face relative to the orbit.
- •
It provides no information regarding the severity of the cleft, only the location.
- •
Orbital hypertelorism refers to true increased distance between the bony orbits.
- •
Surgical repair must be tailored to the individual cleft based on severity and structures involved.
The rarity, complexity, and great variety of craniofacial clefts have all contributed to the difficulty in establishing a concise yet comprehensive classification system for these anomalies. In 1887, Morian proposed a basic schema with the infraorbital foramen as the reference. Morian type I clefts existed in the space between the infraorbital foramen and the facial midline, and type II existed lateral to the infraorbital foramen. Clearly significant ambiguity exists within each of these 2 categories regarding structures involved in the clefting process, and a more precise classification system was needed. Boo-Chai subdivided the oro–ocular clefts described by Morian in an attempt at further refinement, and Karfik was the first to attempt classification by embryologic origin in 1966.
In 1976, Tessier proposed a classification system based on his personal experience with 336 patients, and the resultant ordered numbering system has greatly facilitated communication between reconstructive surgeons. Tessier’s system has gained widespread acceptance and is now the most consistently used method of describing craniofacial clefts in the literature. It is centered on the orbit, with clefts assigned a number in a counterclockwise rotation. Facial clefts are numbered from 0 to 7, with 0 a midline facial cleft, and the cranial clefts are numbered 8 to 14, with 14 being a midline cranial cleft. Midline mandibular cleft is assigned number 30 ( Fig. 1 ). Each of these clefts may involve both soft tissue and bone, and the number does not provide information regarding severity of tissue involvement, merely the location on the face and/or skull.
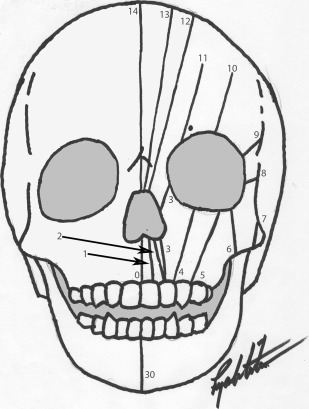
The remainder of this article explores the various Tessier clefts in more detail, followed by a discussion of orbital hypertelorism (an abnormally widened distance between the bony orbits), which may be present in association with some craniofacial clefts.
Tessier 0
Tessier 0 cleft is a true midline facial cleft, which may be accompanied by a Tessier 14 cleft (extension of the midline cleft to the cranium), with a resultant variable degree of hypertelorism. This is among the more common of the “atypical facial clefts,” although it is still very rare, with a incidence reported as 1 in 1 million live births.
Soft Tissue
The subtlest manifestation is a broadening of the philtrum, with a typical bifid nasal tip and columella, which are widened with a central concavity. In more complete cases, a true midline cleft lip may be present. The nose will thus appear shortened, and the nasal ala laterally displaced and the alar base widened.
Bone
The midline cleft alveolus appears between the central incisors ( Fig. 2 ), producing a characteristic sloping alveolar ridges toward the cleft bilaterally, described as keel shaped. This will typically create an anterior open bite deformity from vertical deficiency of the maxilla in the region of the midline cleft. Involvement of the nasal septum is variable, and ranges from mild thickening of the septal cartilage and thickening and flattening of the maxillary crest, to lateral displacement of the nasal processes of the maxilla, to true duplication of the septal structures and significant lateral displacement of the nasal bones.
In severe cases, where the cleft extends superiorly or exists in conjunction with a Tessier 14 cleft, the ethmoid sinuses are volumetrically enlarged and prolapsed inferiorly and laterally. There may be widening of the floor of the anterior cranial fossa and hypertelorism. The sphenoid sinus may prolapse anteroinferiorly, although the body of the sphenoid bone is characteristically normal. The pterygoids may be displaced somewhat laterally.
Tessier 0
Tessier 0 cleft is a true midline facial cleft, which may be accompanied by a Tessier 14 cleft (extension of the midline cleft to the cranium), with a resultant variable degree of hypertelorism. This is among the more common of the “atypical facial clefts,” although it is still very rare, with a incidence reported as 1 in 1 million live births.
Soft Tissue
The subtlest manifestation is a broadening of the philtrum, with a typical bifid nasal tip and columella, which are widened with a central concavity. In more complete cases, a true midline cleft lip may be present. The nose will thus appear shortened, and the nasal ala laterally displaced and the alar base widened.
Bone
The midline cleft alveolus appears between the central incisors ( Fig. 2 ), producing a characteristic sloping alveolar ridges toward the cleft bilaterally, described as keel shaped. This will typically create an anterior open bite deformity from vertical deficiency of the maxilla in the region of the midline cleft. Involvement of the nasal septum is variable, and ranges from mild thickening of the septal cartilage and thickening and flattening of the maxillary crest, to lateral displacement of the nasal processes of the maxilla, to true duplication of the septal structures and significant lateral displacement of the nasal bones.
In severe cases, where the cleft extends superiorly or exists in conjunction with a Tessier 14 cleft, the ethmoid sinuses are volumetrically enlarged and prolapsed inferiorly and laterally. There may be widening of the floor of the anterior cranial fossa and hypertelorism. The sphenoid sinus may prolapse anteroinferiorly, although the body of the sphenoid bone is characteristically normal. The pterygoids may be displaced somewhat laterally.
Tessier 1
A Tessier 1 cleft is similar to a “typical” cleft lip. This is a paramedian cleft in the Cupid’s bow, extending superiorly to the dome of the alar cartilage or even to the medial aspect of the brow. Extension beyond the medial orbit/brow denotes a Tessier 13 cleft, which may exist simultaneously.
Soft Tissue
A paramedian cleft lip is present, extending above the lip into the dome of the alar cartilage. The lower lateral cartilage and alar dome are cleft, with a short, wide columella. The lateral remnant of the ala and lower lateral cartilage may be atrophic, curled, and deviated away from the cleft margin. Extension of the cleft into the upper lateral cartilage and nasal sidewall or paramedian nasal dorsum ranges from subtle furrow in the soft tissue to frank cleft toward the medial brow and orbit. Severe manifestations of the Tessier 1 cleft result in severe telecanthus and a variable degree of true hypertelorism, depending on bony involvement.
Bone
As in “typical” cleft lip and palate, Tessier 1 may extend posteriorly into the maxilla, resulting in a paramedian cleft alveolus or complete cleft palate. There is frequently a partial anterior open bite on the cleft side ( Fig. 3 ), and the maxilla is hypoplastic ipsilaterally, with severe maxillary hypoplasia potentially creating paradoxic choanal atresia. The medial maxillary wall is preserved, although distortion of the nasal septum may flatten the nasal dorsum. There is distortion of the anterior cranial fossa, with relative hypoplasia of the ipsilateral pterygoids and sphenoid wings.
Tessier 2
Tessier 2 cleft is also a paramedian cleft lip with concomitant underdevelopment of the nasal ala on the cleft side. There is no true notching of the ala nasi, helping to distinguish Tessier 2 from Tessier 1. The base of the nose is widened, and the lateral crus of the cleft side lower lateral cartilage is flattened. The root of the nose is also widened and flattened, and bony notching of the nasal bone is present, with resultant hypertelorism. Cranial extension corresponds with Tessier 12. The cleft alveolus is present at the lateral incisor and extends into the pyriform aperture. It does not disrupt the medial wall of the maxillary sinus ( Fig. 4 ).
Soft Tissue
The cleft lip extends into the nostril as a wide cleft, with a flattened and laterally displaced lower lateral cartilage. There is no notching of the cartilage itself. There is a flattening of the nasal dorsum and sidewall, and a soft tissue groove may be present extending to the root of the nose. The eyebrows are intact.
Bone
The alveolar cleft is present in the area of the lateral incisor and extends as a unilateral complete cleft palate. The nasal septum is deviated to the noncleft side and is intact. The cleft side maxilla is hypoplastic, and cases of paradoxic choanal atresia (cleft side and bilateral) have been described. The ethmoid is broadened with resultant orbital hypertelorism, and notching of the nasal bones is present. The ipsilateral frontal sinus is not pneumatized, and the orbit is narrowed.
Tessier 3
As seen in Tessier clefts 1 and 2, there is a paramedian cleft lip. Unlike Tessier 1 and 2, the cleft does not involve the nasal base or lower lateral cartilage. The cleft extends superiorly involving the lower eyelid medial to the punctum ( Fig. 5 ). The medial canthi are disrupted, as is the nasolacrimal system. Concurrent microphthalmia or anophthalmia may be present. The cleft alveolus is more lateral than in the typical cleft palate, coursing between the lateral incisor and canine. The medial wall of the maxillary sinus is absent, and the medial and inferior orbital walls are disrupted, leading to direct communication between the oral cavity, nasal cavity, and orbit. Cranial extension results in Tessier cleft 11.
Soft Tissue
There is extreme vertical soft tissue deficiency of both margins of the cleft, resulting in superior displacement of the alar base and minimal soft tissue present between the alar base and the lower eyelid. The inferior lacrimal punctum is visible at the margin of the cleft eyelid, and the lacrimal sac opens directly onto the cheek and does not communicate with the nasal cavity.
Bone
The alveolar cleft is present between the lateral incisor and canine, and the medial maxillary wall is absent. The maxilla is hypoplastic on the cleft side, and the nasal septum deviates away from the cleft. The cleft may extend superiorly to the medial and inferior orbital walls and onto the inferior orbital rim. This results in communication between the orbit, nasal, and oral cavity. The cleft side pterygoid is displaced medially, and the orbit and floor of the anterior cranial fossa are displaced inferiorly.
Tessier 4
Tessier 4 cleft involves the lip at the midpoint between the commissure and philtral column. It extends onto the cheek, lateral to the alar base and pyriform aperture, and can involve the lower eyelid lateral to the punctum, sparing the nasolacrimal system. The alveolar cleft occurs between the lateral incisor and canine, courses through the maxillary sinus medial to the infraorbital foramen and may involve the medial aspect of the inferior orbital rim ( Fig. 6 ).
Soft Tissue
Similar to the Tessier 3 cleft, there is significant vertical soft tissue deficiency along the margins of the cleft, with the medial margin of the cleft lip extending onto the medial margin of the cleft lower eyelid. The nasal ala is displaced superiorly, and the nose is shortened. Muscle may be congenitally absent in the medial aspect of the cleft lip. Significant vertical dystopia and hypoglobus may be present owing to skeletal deficiencies of the orbital rim and medial orbital wall, although both globes are otherwise normal.
Bone
The alveolar cleft passes between the lateral incisor and canine, extending as a unilateral complete cleft palate. The cleft involves the maxillary sinus, which is hypoplastic, although the medial wall remains intact and extends to involve the inferior orbital rim and floor. Direct communication between the orbit, maxillary sinus, and oral cavity exists, but the nasal cavity is separate. There is severe midfacial hypoplasia, and asymmetry of the sphenoid is present. The cleft does not extend to the skull base.
Tessier 5
The cleft lip originates just medial to the oral commissure, though the commissure itself is uninvolved (distinguishing Tessier 5 from Tessier 7). The cleft extends across the cheek and terminates at the lateral one-third of the lower eyelid. Eye malformations are common, particularly microphthalmia. The alveolar cleft is in the premolar area and extends superiorly to involve the orbital floor and lateral inferior orbital rim ( Fig. 7 ).
Soft Tissue
There is vertical soft tissue deficiency along both margins of the cleft, although it is more severe between the lip and lower eyelid. There is mild shortening of the nose on the cleft side with some superior displacement of the alar base. There is no involvement of the upper eyelid, brow, or hairline and the globes are normal. Vertical dystopia and facial asymmetry are present as a result of underlying bony abnormalities.
Bone
Bony involvement is variable. In mild cases, a simple bony depression exists along the face of the maxilla, whereas in more severe cases, a wide bony cleft is present coursing lateral to the infraorbital foramen and hypoplastic maxillary sinus. This cleft can extend to the lateral inferior orbital rim, although it does not communicate with the inferior orbital fissure. There is a shortening of the lateral orbital wall and greater wing of the sphenoid. The cleft side pterygoid plates are medialized and underdeveloped.
Related posts:



Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


