This article reviews evaluation and techniques for neck rejuvenation. It includes a detailed overview of cervical rhytidectomy and discusses the potential complications associated with surgical correction. A review of clinical outcomes in the literature is also included.
Key points
- •
It is imperative to identify the goals of the patient and his or her desired outcome.
- •
Careful examination of the patient is important to determine if correction can meet the patient’s goals.
- •
Surgical correction is focused on re-establishing the cervicomental angle, decreasing submental fullness, eliminating jowls, and platysmal banding.
- •
There are multiple adjuvant procedures that can be employed to augment surgical correction.
- •
Surgical correction is not without risks, and complications include hematoma, nerve injury, flap necrosis, and scar irregularities.
Introduction
Aesthetic rejuvenation of the neck focuses on restoring the shape and contour of the neck, with special attention to redefining the cervicomental angle. As individuals age, the neck skin loses elasticity; submental fat becomes abundant and ptotic, and the platysmal muscle adherence to the subplatysmal fat and tongue musculature weakens. Additionally, muscle tone atrophies, and the submandibular glands descend. As a result, the cervicomental angle becomes blunted; the angle and inferior border of the mandible lose definition, and there is an abundance of skin in the submentum. These changes embody individuals’ dissatisfaction with the appearance of their neck and their desire to seek surgical correction. Various surgical and nonsurgical techniques are used alone or in combination to address the aging process of the neck and deliver the desired result of restoration.
Introduction
Aesthetic rejuvenation of the neck focuses on restoring the shape and contour of the neck, with special attention to redefining the cervicomental angle. As individuals age, the neck skin loses elasticity; submental fat becomes abundant and ptotic, and the platysmal muscle adherence to the subplatysmal fat and tongue musculature weakens. Additionally, muscle tone atrophies, and the submandibular glands descend. As a result, the cervicomental angle becomes blunted; the angle and inferior border of the mandible lose definition, and there is an abundance of skin in the submentum. These changes embody individuals’ dissatisfaction with the appearance of their neck and their desire to seek surgical correction. Various surgical and nonsurgical techniques are used alone or in combination to address the aging process of the neck and deliver the desired result of restoration.
Treatment goals and planned outcome
The primary goal of surgery is to restore the youthful appearance of the neck. This includes re-establishing a refined cervicomental angle, decreasing adiposity and fullness in the submentum, obliterating platysmal banding, eliminating jowling, and recreating definition of the mandible. Multiple studies have defined the appearance of a youthful neck. Some of the characteristics include an acute cervicomental angle between 105° and 120°, a distinct inferior border of the mandible, visible anterior borders of the sternocleidomastoid muscles, and a noticeable thyroid cartilage and subthyroid depression.
Baker has developed a classification system of the aging process in the neck and lower face. This organizes patients into 4 subtypes based on the severity of the jowl and neck. Type 1 patients have slight cervical skin laxity with submental fat and early jowls. Type 2 patients have moderate cervical skin laxity, moderate jowl, and submental fat. Type 3 patients have moderate cervical skin laxity, but with significant jowling and active platysmal banding. Type 4 patients have loose, redundant cervical skin and folds below the cricoid, significant jowls, and active platysmal bands.
Classification systems as the one described can categorize patients and help to highlight the key anatomic findings of different patients and their primary need for rejuvenation. It is important to distinguish the need for correction so that the correct method of neck rejuvenation can be used to target the specific anatomic finding. There are many methods that have been described for neck rejuvenation. Many of these are variants on larger themes and include both surgical and nonsurgical options. These range from chemodenervation, laser skin resurfacing, submental liposuction, skin tightening procedures, skin excision procedures, platysmaplasty, suspension sutures, and digastric modification. It is important to identify the need for correction as well as the patient’s goals of surgery to determine the best course of rejuvenation.
Ideal candidates for surgery are patients with strong bone structure with a normal position of the hyoid bone and good chin projection, as well as skin of medium thickness that has maintained its elasticity. Certain anatomic considerations can alter the potential outcome. Obtaining a sharp cervicomental angle can be hampered in patients with low positioned hyoid bones as well as retrognathic patients. There is little that can be done in the patient with a low positioned hyoid bone, but in the retrognathic patient, augmentation mentoplasty should be considered. Neck definition can also be suboptimal in patients with thick skin or excessive subcutaneous adiposity.
This article addresses cervical rhytidectomy as well as adjuvant techniques that can be employed to reach the desired goal of the patient and surgeon.
Preoperative planning and preparation
Prior to consultation, the patient is asked to fill out a detailed questionnaire. Routine historical questions are asked to obtain information about their medical, surgical, social, and family history. On the day of the initial consultation, patients are photographed for documentation and to aid in preoperative planning. The standard photographic views include full-face frontal view, right and left oblique views, and right and left lateral views. All photographs are taken in the Frankfurt horizontal line using a single lens reflex (SLR) with appropriate medium blue background and balanced cross-lighting.
It is imperative to determine the patient’s goal and desire for correction and to define which modality of correction will target and correct his or her desire for rejuvenation. For instance, if a patient’s primary concern is an abundance of submental adiposity and mild jowling, but the patient has maintained skin elasticity, submental lipectomy would be a reasonable approach versus cervical rhytidectomy. However, for patients with blunting of anatomic landmarks and redundant ptotic cervical skin, a cervical rhytidectomy is the most reasonable approach.
A complete medical history should be obtained. Patients with a history cardiovascular disease are not precluded from surgery but require preoperative clearance by their cardiologist. Also, the overall health and ability of the patient to tolerate anesthetic and surgical intervention should be assessed. All patients are given an American Society of Anesthesiologists (ASA) classification. There are not many systemic diseases that proscribe patients from cervical rhytidectomy. Relative contraindications to surgery include advanced autoimmune diseases relating to the skin of the face, a history of systemic isotretinoin use, and medications or true allergy that would impact the ability to use local anesthetic. Obesity is not a contraindication to surgical correction; however, if a significant weight loss is planned in the near future, it is advised that surgery is postponed until after the patient’s desired weight has been achieved. A history of full-course radiation treatment to neck and preauricular area is an absolute contraindication to cervical rhytidectomy. The physical examination should be focused on the neck and jaw line. The quality of the skin is assessed, including thickness, degree of elasticity, and severity of dermatochalasis. Skin laxity in the jowl, submental, and cervicomental angle is also evaluated. The position of the hyoid bone and chin position is noted. Identifying these key findings allows the surgeon the opportunity to discuss potential limitations of surgical correction and ensures the patient has reasonable postoperative expectations.
All of the patient’s questions should be answered. The procedure should be outlined in detail, including incision placement. The risks, benefits, potential complications, alternatives and limitations must be comprehensively discussed prior to conclusion of the consultation. All patients undergoing surgery should be asked to suspend all anticoagulants and vitamin supplements that may cause clotting abnormalities prior to surgery.
Patient positioning
On the day of surgery, the planned incision lines are marked with patient in the upright and seated position. The incision is placed in a trichophytic fashion at the temporal and postauricular hairline. This location is chosen to avoid elevating the hairline following redraping of the skin. The senior author (EHF) does not change the position of the incision in male patients. The submental incision is marked as well and is always posterior to the natural chin crease to decrease visibility postoperatively.
The patient is placed supine on the operating table. Although patients are given the option of anesthesia, most patients choose a general anesthesia. Following intubation, 2 to 3 mm of hair is trimmed along the planned incision lines. The hair is then sectioned and secured with rubber bands around the planned incisions.
Procedural approach
Neck Lift Procedure
A modified tumescent solution is prepared of 0.1% lidocaine with 1:1,000,000 epinephrine. The neck skin is infiltrated with 70 to 80 mL prior to beginning the procedure.
The procedure begins with a submental incision approximately 3 cm in length placed posterior to the natural submental crease. Placement of the incision here prevents scar contraction and unsightly postoperative deformity. A skin flap is elevated in the subcutaneous plane, extending inferiorly below the thyroid notch and laterally to the submandibular glands.
If the patient has excessive submental fat, this should be directly excised or aspirated. Subplatysmal fat should not be removed to prevent postoperative platysmal banding. A decision should then be made regarding need for platysmaplasty. Indications for platysmaplasty include severe preoperative platysmal banding and cobra neck deformity. If indicated, the plastysma muscle is elevated from the underlying tissue inferiorly to the hyoid bone. The platysma muscle is divided at the level of the hyoid bone or desired position of the cervicomental angle to recreate that angle. Historically, the senior author (EHF) has performed midline platysmal imbrication at this point; however, more recently, this has been abandoned to favor superolateral (rather than medial) vectors of motion. Hemostasis is then obtained with electrocautery. Once hemostasis has been achieved, the submental incision is closed with deep buried interrupted sutures.
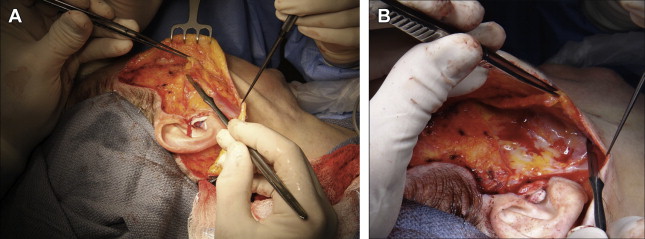
Attention is then paid to the right side of the face. An additional 70 to 80 mL of 0.1% lidocaine with 1:1,000,000 epinephrine is infiltrated into the subcutaneous plane of the right-sided neck lift flap and incision. The postauricular incision is made, and skin flap elevation is performed sharply. The skin flap is elevated anteriorly using blunt dissection with scissors. A temporal trichophytic and tragal preauricular incision is then made, and the short skin flap is elevated anteriorly. A preauricular strip of areolar tissue and fat is trimmed from the zygomatic arch superiorly to approximately 2 cm below the angle of the mandible to delineate the posterior extent of the superficial musculo-aponeurotic system (SMAS) flap. The superior extent of the SMAS flap is made by drawing the scalpel laterally from the inferior orbital rim to the tragal cartilage ( Fig. 1 ). The deep plane is then elevated deep to the platysma muscle but superficial to the masseteric fascia ( Fig. 2 ). The marginal mandibular branch of the facial nerve is identified and protected during the dissection. The deep plane is suspended to the root of the lateral orbital rim, zygomatic arch, the mastoid cortex, fascia of the sternocleidomastoid, and preauricular soft tissue with a combination of permanent and slow-absorbing sutures. Hemostasis is achieved with electrocautery. The skin flap is then redraped ( Fig. 3 ), marked, and all redundant skin excised. The skin flap is closed in layers with multiple deep buried interrupted sutures, and the epidermis is reapproximated with a fast-absorbing suture. An identical procedure is performed on the contralateral side. At the conclusion of the procedure, a pressure dressing is applied prior to extubation.
Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


