Techniques for Controlling Tip Rotation in Open Rhinoplasty
Nicolas Tabbal
Geo N. Tabbal
DEFINITION
Nasal tip rotation can be assessed in various ways, but the nasolabial angle is the preferred measurement. It is defined as the angle formed by the intersection of a line between the most anterior and posterior points of the nostril and a line perpendicular to the horizontal facial plane (FIG 1). Tip rotation determines nasal length; increasing tip rotation (larger angle) shortens the nose, and decreasing tip rotation (smaller angle) lengthens the nose.
A nasolabial angle of 95 to 110 degrees in women and 90 to 95 degrees in men is frequently cited as ideal, but a variety of cultural, ethnic, and other influences are taken into consideration.
Increasing tip rotation entails cephalad rotation of the tip, thereby increasing the nasolabial angle and shortening the nose by decreasing the distance between the radix and the tip-defining points.
Decreasing tip rotation results in a decreased nasolabial angle and lengthening of the nose as the distance between the radix and the tip-defining points increases.
ANATOMY
Tip position results from the interplay between cutaneous attachments to the cartilaginous framework, fibrous attachments between the upper and lower cartilages, abutment of the lower lateral cartilages (LLCs) against the piriform aperture, prominence of the caudal septum, location and attachment of the medial crura and the caudal septum, length of the upper lateral cartilages, and location of the anterior septal angle.
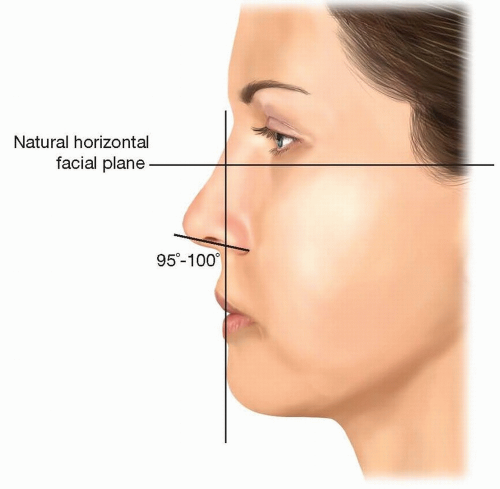 FIG 1 • Analyzing tip rotation by measuring the nasolabial angle. |
PATIENT HISTORY AND PHYSICAL FINDINGS
Physical inspection of the external nasal features and an intranasal evaluation using a speculum and light source are necessary to construct a treatment plan.
Ballottement of the nasal tip provides information about tip support.
Assessment of skin thickness helps determine the degree of cartilage modification required to achieve the desired result.
Standard medical photography should include standard rhinoplasty views such as the frontal, lateral (ie, profile), basal, and oblique views.
Many patients present with complaints of tip descent on animation, suggesting that the action of the depressor septi nasi is causative for this dynamic rotation of the nasal tip (FIG 2). Recent studies contradict this mechanism and suggest that the tip does not move significantly on smiling, but rather the alar bases are pulled cephalad, creating the appearance of a plunging tip.
IMAGING
Standard 2D medical photography is necessary for accurate preoperative analysis, intraoperative decision-making, and assessing postoperative outcomes. In addition, the surgeon may choose to use an imaging system to aid in communicating desired postoperative outcomes.
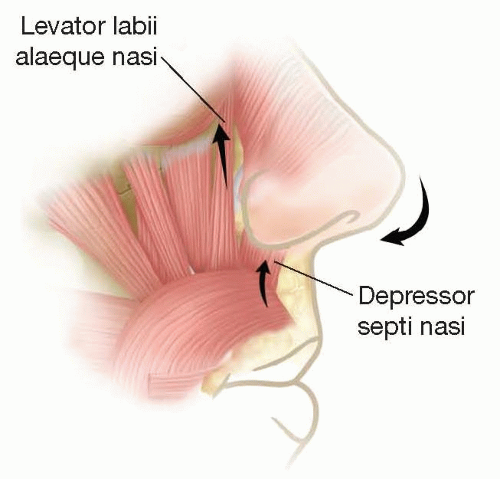 FIG 2 • The depressor septi nasi muscle draws the tip down with animation. |
SURGICAL MANAGEMENT
The first step in any surgical procedure, and particularly in rhinoplasty, is an accurate diagnosis.
Patients’ expectations and surgeons’ views on surgical limitations must be effectively communicated. No patient will get the exact nose that he or she wants.
Preoperative Planning
Prior to infiltration with local anesthetic, a more thorough intranasal examination is performed to confirm that the preoperative plan is accurate and feasible.
Positioning
The patient is placed supine on the operating table with the vertex of the scalp located just beyond the end of the bed.
After intranasal intubation or placement of a laryngeal mask airway, the eyelids are taped shut with tape placed sufficiently far laterally to not interfere with the procedure.
A throat pack is inserted.
Oxymetazoline-soaked pledgets may be placed in each nare with the aid of a nasal speculum and a headlight for accurate placement. There is no role for cocaine in rhinoplasty.
The nasal framework is infiltrated with local anesthetic that includes epinephrine.
Approach
The debate over the open vs closed approach continues. Any technique for tip rotation is more easily and, by most surgeons, more accurately performed using the open approach. The exposure is better, and the ability to fix the tip in the desired position and to keep it there is also better.
The closed approach is reasonable when the tip rotation will not be altered significantly, but, even then, one must be willing to convert to an open approach if the desired tip rotation/projection cannot be achieved.
TECHNIQUES
▪ Skin Undermining
The attachments between the tip cartilages and the skin restrict the rotation of the nasal tip and are effectively released when initial exposure is obtained whether the approach is open or closed.
▪ Division of the Scroll Area
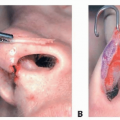
Release of the fibrous, or sometimes cartilaginous, attachments between the lateral crura and the upper lateral cartilages is necessary to rotate the tip and is achieved by performing a cephalic trim. If no cephalic trim is performed, then an intercartilaginous incision or division of the scroll area is necessary. In cases when significant tip rotation is performed, an intercartilaginous incision may be necessary in addition to the cephalic trim to maximally liberate the lateral crura. Similarly, division of the attachments between the medial crura and the caudal septum is necessary for significant tip rotation (TECH FIG 1A).Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree