30 Tattoo Removal with Lasers
The growing trend of tattooing has led to increased numbers of patients seeking tattoo removal. Studies note that 40% of Americans between the age of 26 and 40 currently have tattoos and 17% of these people are seeking removal.1,2 With more than 20,000 tattoo studios in the United States placing tattoos, the demand for removal is likely to continue to increase in the coming years.3
Multiple techniques can be used for tattoo removal. Early removal methods used mechanical destruction such as dermabrasion, chemical peels, and continuous-wave lasers. These methods left patients with unsatisfactory results and were associated with suboptimal removal and scarring (Figure 30-1). The current standard of using Q-switched lasers has revolutionized tattoo removal and offers patients a safe and effective means for removing tattoo ink.

FIGURE 30-1 Dermabrasion results for tattoo removal showing scarring, hypopigmentation, and residual ink.
(Copyright Rebecca Small, MD.)
Tattoo Anatomy
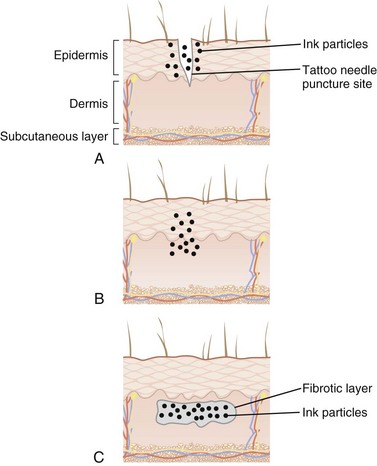
During the tattooing process, tattoo ink is injected intradermally. The epidermis and upper papillary dermis are homogenized and ink particles (ranging in size from 2 to 400 nm) are deposited intracellularly and extracellularly. After 2 to 3 months, the skin layers are reestablished and ink is concentrated in the dermis within fibroblasts, beneath a layer of fibrotic scar tissue (Figure 30-2).
Laser Principles
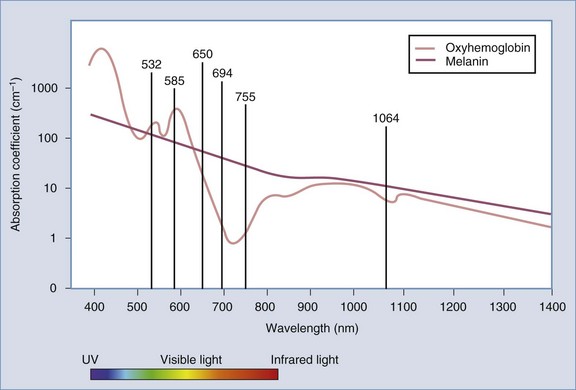
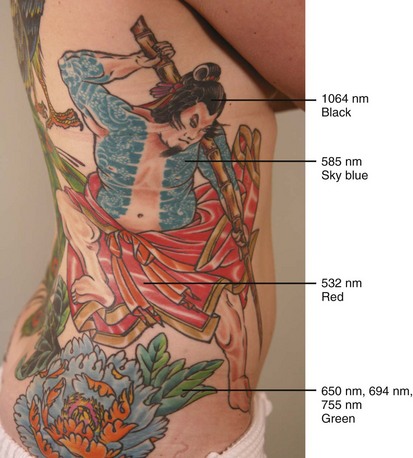
Tattoo ink serves as a cutaneous chromophore for lasers. Certain wavelengths of light are selectively absorbed by different ink colors.4 In this way, colored inks can be targeted and removed by laser light with minimal damage to surrounding tissues. The chromophore absorption spectrum of the tissue chromophores, melanin and oxyhemoglobin, as well as wavelengths used for tattoo removal, are shown in Figure 30-3. Wavelength selection for different tattoo colors is shown in Figure 30-4 and is as follows:
Laser parameters including wavelength, pulse duration, and fluence can be tailored to maximize tattoo ink destruction and minimize thermal damage to surrounding tissue. Short pulsed, Q-switched lasers further employ photoacoustic vibration to fragment tattoo ink into smaller particles. These smaller ink particles are eliminated through epidermal extrusion, lymphatic drainage, and macrophage phagocytosis. In addition, laser-treated ink particles have altered optical properties that render the ink remaining in the skin less visible to the eye.5
Laser Parameters and Tattoo Treatments
Patient and Tattoo Selection
Almost any tattoo is indicated for laser tattoo removal. Multiple treatments are needed to achieve satisfactory results. Due to great variation in tattoo ink depth, density, composition, and techniques used for placement, the number of treatments needed for removal can be difficult to estimate accurately. In general, professionally placed tattoos have a high ink density and require 9 to 14 treatments, whereas amateur tattoos typically require 4 to 8 treatments. Several other factors can affect the number of treatments necessary for removal: faded, older tattoos on paler skin types in more proximal locations tend to resolve with fewer treatments than intense, multicolored tattoos on darker skin types in distal locations.6 Patients should be questioned about other tattoo removal methods used previously. Methods that create scar tissue, such as burning or abrasion, can make tattoo removal with lasers less successful.
Alternative Therapies
The following alternatives to Q-switched laser tattoo removal methods are not recommended:
Products Currently Available
The Q-switched Nd:YAG (neodymium-doped yttrium aluminum garnet) produces a 1064 nm wavelength of light that is ideal for treating black ink. A primary disadvantage is its limited efficacy in removing yellow and green inks. With some devices, through a process called frequency doubling, an Nd:YAG laser can also produce light with a wavelength of 532 nm to treat red, orange, and yellow inks.20 The Nd:YAG laser has an advantage of treating darker skinned patients with less risk of hypopigmentation, hyperpigmentation, and textural changes.7 This can be attributed to the increased dermal penetration of this longer wavelength and the lower melanin absorption. The wavelength of the light emitted by the Q-switched alexandrite laser is 755 nm. This wavelength has excellent absorption by black, good absorption by green and blue, but poor absorption by red ink. The ruby laser was one of the first Q-switched lasers, and it emits a 694 nm wavelength. It works well for darker colors (black, blue-black, and some green), but poorly on yellow and red ink. Although more effective for green ink than the Nd:YAG, the ruby laser commonly causes hypopigmentation and hyperpigmentation and, although usually transient, may be permanent.5
Contraindications8
Also see Chapter 26, Hair Reduction with Lasers, for additional laser contraindications.









