9Surgical Treatment of Rhinogenic Migraine Headaches (Site III)
Bahman Guyuron
Salient Points
• Many of the daily migraine headaches (MHs) have a rhinogenic origin.
• Prolonged supine position, low atmospheric pressure, and hormonal changes can trigger rhinogenic MH.
• Erect position, spraying vasoconstrictors intranasally, and increases in atmospheric pressure can reduce rhinogenic MH.
• The pain is usually behind the eyes and can extend to the temples, forehead, or even occipital areas.
• Computed tomography scan findings may include a large spur touching the turbinates or even the sidewall of the nose, concha bullosa, paradoxical curl of the turbinates, or Haller’s cell.
• The surgery is completed under general anesthesia as an outpatient procedure.
• The septoplasty is performed through an L-shaped (Killian) incision, if needed.
• The surgical goal is to eliminate the contact points and decompress the concha bullosa, Haller’s cell, or remove the paradoxical curl.
• The deviated portion of the septal cartilage is removed leaving as much of the straight portion of the septal L frame as possible, a minimum of 20 mm anteriorly and 10 mm caudally.
• It is always easier to elevate the posterior portion of the periosteum and extend the dissection anteriorly along the floor on each side of the vomer bone.
• The deviated portion of the vomer bone and the ethmoid plate are removed using a double-action rongeur.
• It is crucial to examine both sides of the nasal cavity thoroughly to assure that the spur and the deviated portion of the septum are removed completely.
• The medial wall of the concha bullosa is removed using a number 4 XPS shaver or with a rongeur.
• The remaining portion of the turbinates is gently cauterized, sprayed with thrombin solution, or both.
• The straight portion of the removed septal cartilage is replaced between the mucoperichondrial layers prior to the repair of the L incision with 5-0 chromic running suture.
• Doyle stents are placed in position and fixed to the membranous septum with 5-0 Prolene suture and kept in place for a minimum of 4 days.
9.1 Introduction
The septum and turbinates are common migraine headache (MH) trigger sites. Frequent occurrence of other headaches arising from this site creates a challenge in differentiating rhinogenic MH and other sinus- and septum-related headaches. Many of the chronic daily MHs with retrobulbar pain emerge from this site. When one considers the anatomical reasons for headaches arising from this trigger site, which is often contact between the septum and the different turbinates, it becomes easy to understand why these patients have daily MH, since the contact is often continuous and thus the headache is relentless.
The patients with rhinogenic MH invariably experience pain behind the eyes, although occasionally it can be felt in the cheek area or even the nasal bones. Commonly, the patients have nausea and vomiting associated with photophobia and phonophobia in addition to the headaches. These symptoms could serve to differentiate MHs from sinus-related headaches. The patients frequently wake up in the middle of the night or in the morning with headaches since prolonged supine position may result in more intense contact sites. The association between atmospheric pressure changes and headaches is so powerful that many of these patients can actually predict the weather changes with impressive accuracy. Additionally, there is a very close connection between rhinogenic MHs and hormonal changes. This is why patients may experience headaches during menstruation. Furthermore, many of the cluster headaches are connected with abnormalities in this site, as we have discussed previously. When one considers the commonality between recumbent position, hormonal and weather changes, and MH, it becomes clear that during all of these conditions, the contact between the turbinates and septum becomes intensified due to enlargement of the turbinates. Some of these patients can ratify that when they stand up or sit up after being awakened by the headaches, the pain can be mitigated. Similar improvement in MH can be noticed when the patient uses nasal decongestants. The explanation is that being in an erect position or use of decongestants reduces the size of the turbinate; thus, the intensity of the contact between the turbinates and the septal spur is diminished, and the headaches often cease or lessen.
The diagnosis is easy with review of the computed tomography (CT) scan images, which provide clear objective evidence. The abnormalities commonly seen in the CT scan include a large spur touching the turbinates or even the sidewall of the nose, concha bullosa, paradoxical curl, or Haller’s cell. A small percentage of patients also have chronic sinus disease with thickening of the lining in the sinuses. Reviewing the CT scan with the patients, notwithstanding their medical background, increases the patient’s confidence in the surgical plan immeasurably since the patients can easily visualize the abnormalities that are pointed out by the surgeon. The presence of strong symptoms of airway occlusion plays a paramount role in the decision to operate on the septum and the turbinates in patients with insufficient evidence for the nose being an MH trigger site. It is advisable to combine the septoplasty and turbinectomy with deactivation of the other trigger sites in this group of patients with the primary goal being improvement in the airway and the improvement of MH being a secondary goal.
9.2 Surgical Technique
The surgical correction will depend on the CT scan findings and symptomatology. The majority of these patients would be candidates for a septoplasty. In fact, of all the intranasal techniques that are available, septoplasty will probably yield the most benefit to the patient, even if the other pathological findings are not eliminated. A properly done septoplasty will take away the rigid wall or spur that is in contact with the turbinates, thus reducing the impact of the contact. However, combining the septoplasty with reduction of turbinate on the contact area offers a higher level of confidence for success.
Surgery is invariably performed under general anesthesia as an outpatient operation. Although topical anesthesia enforced with injection of local anesthetic could be sufficient for minor procedures, it is not an optimal way of dealing with the major intranasal pathology. Under most scenarios, general anesthesia is preferred. The nose is infiltrated with Xylocaine containing 1:100,000 epinephrine along the sidewalls, the dorsum, the roof, and floor of the nose. Topical application using pads saturated with anesthetic and vasoconstrictive agents such as neo-synephrine will further reduce the vascularity and intensify the vasoconstrictive effect of the injected materials. The turbinates are injected with Xylo-caine containing 1:100,000 epinephrine.
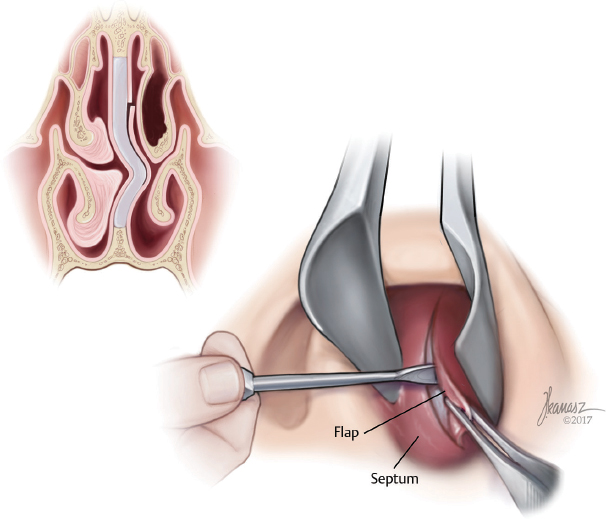
Septoplasty is performed through an L-shaped (Killian) incision. The incision is made on the left side by a right-handed surgeon (►Fig. 9.1). The mucoperichondrial flap is elevated on the left side of the septum (►Fig. 9.2). The incision is then taken through the septal cartilage only using the sharp end of the septal elevator to avoid penetration of the right side mucoperichondrium (►Fig. 9.2). The mucoperichondrium on the right side of the septum is elevated posteriorly, extending to almost the nasopharynx and posterior wall of the nose. The dissection is also continued along the caudal portion of the cartilage and septum, the vomer plate, and perpendicular plate of the ethmoid bone. It is always easier to elevate the posterior portion of the periosteum and extend the dissection anteriorly along the floor on each side of the vomer bone (►Fig. 9.3). The septal cartilage incision is then extended to the ethmoid bone (►Fig. 9.4). At this level, using the sharp end of the septal elevator, the quadrangle septal cartilage is gently pried away from the perpendicular plate of the ethmoid bone (►Fig. 9.5). This dissection is continued posteriorly and caudally at the junction of the vomer bone and the cartilage in a step-by-step fashion until the cartilage is completely free. The cartilage is then removed leaving as much of the straight portion of the septal L frame as possible, a minimum of 20 mm anteriorly and 10 mm caudally (►Fig. 9.6). This will expose bony irregularities and spurs to their fullest extent. The deviated portion of the vomer bone and the ethmoid plate are removed using a double-action rongeur (►Fig. 9.7). It is crucial to examine both sides of the nasal cavity thoroughly to assure that the spur and the deviated portion of the septum are removed completely. The straight portion of the removed septal cartilage is placed back in position and the mucosa incision is repaired using 5-0 chromic running, quilting suture (►Fig. 9.8; also see ► Video 9.1). The mucosa incision is repaired using 5-0 chromic running, quilting suture (►Fig. 9.9).