24 Surgical Treatment for Lower Extremity Lymphedema
Summary
Physiologic surgical treatment for lymphedema includes lymphovenous anastomosis, lymph node transfers, and lymph vessel transplantation. With these physiologic approaches, lymphedema can be treated by reestablishing the drainage of lymphatics of the extremity.
Keywords: lymphedema, lymphovenous anastomosis, lymph vessel transplantations
24.1 Introduction
24.1.1 History of Lymphatic Channel and LVA
The description of the lymph duct began with the coinage of the word “white blood” by Hippocrates in the 5th century BC. The nature of lymphatic vessels was first revealed by Gasparo Asellius (1581–1626) of the University of Pavia, Pavia, Italy. Asellius, while dissecting a dog immediately after it had been fed, observed a series of vessels filled with a white milky fluid in the peritoneum and intestines. He misunderstood this as a blood vessel leading to the liver and named it the “chilo-duct.” From the 1600s, the anatomy of lymphatic vessels using mercury began and its detailed distribution became clear. In Japan, Genpaku Sugita et al listed lymphatic vessels for the first time in 1774 in the new anatomical book “Kaitai Schinsyo” translated from Dutch to Japanese. Professor Buntaro Adachi, Kyoto University’s first anatomy professor, was passionate about the study of lymphatic vessels, and his successor Professor Shogo Funaoka performed lymphangiography in rabbits for the first time in the world and published it as a German paper in 1929. Furthermore, in 1969 Dr. Yamada of Nagoya University performed a lymphaticovenular anastomosis (LVA) in a dog and patients with lymphedema using a microscope. Efforts of the pioneers in Japan have led to the current treatment of lymphedema.
About 1988, Professor O’Brien (Melbourne) was the only person who performed lymph bypass surgery for the treatment of lymphedema.1 This method had already been tried by many surgeons, but found to be ineffective. In his last speech on lymphedema for us, O’Brien expressed unhappiness at the fact that there were no followers of surgical treatment of lymphedema. This has been the motivation for Dr. Koshima to continue the use of surgery for the treatment of lymphedema since 1990.2,3 Around 1980, the authors developed supermicrosurgical techniques that have made possible the anastomosis of more precise vessels of 0.3- to 0.8-mm caliber size. This technique allows the use of 12–0 nylon with a 50- to 30-μm needle in vascular anastomosis of vessels less than 0.8 mm in diameter. Even in legs with lymphedema of long duration, we found that there remain a sizable number of precise lymphatics and subdermal venules (0.5 mm). With the supermicrosurgical techniques, anastomosis of precise lymphatics and the subdermal venular system with a higher patency rate is possible. The application of these techniques to the drainage of lymphatic fluid into the subdermal precise venular system (LVA) has been achieved with improved results. Since 1990, the authors have performed LVA in 2,000 patients including primary edema of the legs (300 upper arms and 1,700 legs) under local anesthesia. As a result, complete recovery and/or remarkable improvement was obtained in mild and moderate cases with primary edema,2,3 and now new strategies combining LVA with functional lymph channel transfers are established for severe cases with primary edema.
24.2 Definition of Lymphedema
Lymphedema is a disorder of the lymphatic transport caused by congenital abnormality and acquired injury of the lymphatic system, resulting in pathological excessive accumulation of lymph fluid in the interstitial space. If this condition persists, fibrous tissue and adipose tissue will proliferate secondarily. Lymphedema is distinguished from physiological “swelling” caused by retention of lymph fluid after standing for a long period of time.
24.3 Classification
From the cause of its onset, it is classified as (1) primary (idiopathic) lymphedema and (2) secondary lymphedema.
24.3.1 Primary (idiopathic) Lymphedema
• Congenital edemas are those already developed at birth. Sometimes, there is an example showing unilateral seminal edema including the face. There are cases in which edema of the limb is combined with neonatal thoracic fluid and ascites, often complicating protein leaky gastroenteropathy. Although it was considered a congenital edema up to now, the authors believe this is the secondary because it is caused by stenosis or obstruction of the thoracic duct. Hereditary lymphedema (Milroy disease) is congenital edema of both lower limbs and is a rare disorder with autosomal dominant inheritance without other anomalies. Recent developments in molecular biological techniques have revealed vascular endothelial growth factor receptor 3 (VEGFR3), which is responsible for establishing the causative gene and expression of vascular endothelium. This makes it possible to perform genetic diagnosis and it is said to recognize Ala → Thr mutation in exon 18 constituting the kinase domain of VEGFR3.
• Delayed edemas: As for these idiopathic edemas, lymphatic vessels always exist when they are confirmed by surgery. The existence of congenital missing or obstruction (hypoplasia) of thoracic duct is also conceivable, but the details are unknown at this time.
24.3.2 Secondary Lymphedema
Depending on the cause of the condition, it is subdivided as follows:
• After treatments for malignant disease: onset after lymph node dissection and radiotherapy and/or chemotherapy.
• Those accompanying progression and recurrence of malignant tumor: so-called malignant lymphedema.
• Trauma: damage of lymphatic vessel, or extensive scarring.
• Infections: filariasis, etc.
Secondary edema is lymphedema of the limbs after the surgery for breast or uterine cancers, and most cases in the upper limb are secondary. In the lower limb, 87% of the cases are secondary after uterine cancer surgery, but there are male cases, such as after testicular tumor resection. In the lower extremity cases, 29% of cases are bilateral and tend to progress from one side to both sides.
24.4 Stage of Lymphedema
Recently, advanced stage classification of edema for surgical treatment is beginning to be used frequently.
• Stage I: reversible edema in the initial state.
• Stage II: irreversible persistent edema.
• Stage III: sustained progressive edema (often accompanied by acute lymphangitis or cellulitis).
• Stage IV: elephantiasis.
• Stage V: critical edema (septic shock).
Normally, it is considered that after the second phase, it is an indication for compression therapy, and stages II to IV are indication for lymphaticovenous anastomosis. The authors believe all stages are indicated.2,3
24.5 Symptoms and Complications
Redness of the affected limb is a common symptom in the majority of cases. It is mild when getting up; swelling increases when the patients work in the standing position or in the evening. For this reason, many refractory cases are males who cannot get enough resting time. Patients have a fever about once a month to once a year (especially in the summer), and the occurrence of inflammatory symptoms like cellulitis or erysipelas is the most serious complication. The longer the repetition of this, the stronger the fibrosis of the subcutaneous tissue. In the cases where no treatment was given for a long period of time, some become typical elephantiasis. Other frequent complications are tinea and/or ingrown toe nail, requiring treatment with phenol or antifungal topical medication. Frequent complications are lichen planus of the lower leg and edema of the genital region. In the edema of the genital region, some refractory pudendal skin lymph fistula is followed. In the cases of edema of the lower limb after treatment of uterine cancer, treatment including mental care is necessary because there are significant quality of life disorders such as sexual dysfunction due to vaginal stenosis resulting from irradiation failure and pudendal edema. Protein-losing gastroenteropathy associated with obstruction of thoracic duct complicates hypoproteinemia and may have growth disorders in the cases with congenital lymphedema.
24.6 Diagnosis
Although the definite diagnosis method is a classical “lymphangiogram,” it has now become unpopular because it involves incision of the skin of the affected limb and injecting the contrast medium directly into the lymphatic channel. “Lymphoscintigraphy” using isotopes cannot confirm the state of fine lymphatic vessels. Ultrasound, CT, and MRI examination are useful for easily diagnosing the state of edema. Since lymphatic vessels are not confirmed directly, we do not know the site of lymphatic obstruction or condition of lymphatic damage, but we can sufficiently confirm the distribution of moisture in the subcutaneous tissue and the degree of increase in fibrosis and adipose tissue. Moreover, if the Doppler method is used, the presence or absence of merger of venous disease (especially deep venous thrombosis) can also be confirmed. The photodynamic eye method is currently being used clinically and is expected to be promising. Since indocyanine green (ICG) emits fluorescence when it is injected intradermally and then infrared rays are applied, the remaining drainage function can be confirmed with the distribution of ICG incorporated in the lymphatic vessel.4
24.6.1 Differential Diagnosis
It is important to distinguish it from other systemic diseases that cause edema (heart failure, renal failure, hepatic disorder, etc.). Other diseases include the following:
• Deep vein thrombosis: The onset is rapid, unilateral, painful, and often complicates varicose veins, congestive dermatitis, pigmentation, and ulcer.
• Lymphatic malformation (lymphangioma): There is no difference in the degree of edema in the morning and evening and no acupressure trace on the lesion.
• Transient swelling: Swelling at the distal side of the lower leg appears especially in the evening due to prolonged standing and sitting, and the swelling disappears in the morning.
• Lipodystrophy (fat hyperplasia due to abnormal fat metabolism): It is usually symmetrical and does not cause infection without skin hardening.
• Lymphangiosarcoma (Stewart–Treves syndrome): In long-term lymphedema cases (about 10 years), injured lymphatic endothelial cells develop to highly malignant lymphangiosarcoma. Superficial erythema progressively expands, but this noninflammatory legion resists the treatment by antibiotic and therapeutic agents for skin diseases.5 Lymphovenous bypass surgery has now become absolute indication to cure sarcoma (surgical anticancer immune therapy).
24.7 Treatments
• Compression by elastic stocking: It is used to increase tissue pressure by applying external pressure and to prevent exacerbation of edema. Patients must wear it especially when they need to stand for a long period of time in the daytime. Because it is washed frequently, it loosens up in a short period of time; so, it needs to be changed frequently, and stockings must be made to suit individual’s needs with attached chucks, rubber, etc. There is a special order item for those larger than the standard size.
• Skin resection/skin grafting (Charles method, Sistrunk method, Thompson method)6: It is a method of extensive resection of diseased tissue. Although it is effective immediately after surgery, it is said that there are many cosmetic problems such as hypertrophic scars in the long term and recurrence of edema in the resected area.
• Liposuction: It is a method of aspirating fat of the edema part with a liposuction device. Improvement is seen immediately after surgery, but the effect tends to decrease within a few months. Based on the authors’ experience, liposuction shows good results only for the effective cases with lymph bypass surgery.
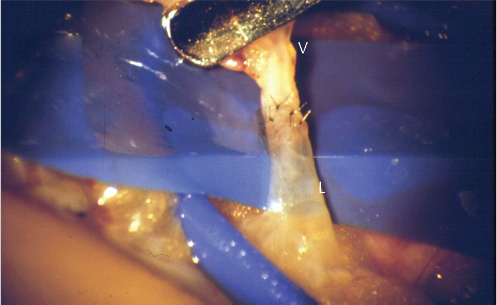
• Lymphovenous anastomosis (LVA; lymph bypass surgery): Operative treatment was applied to all patients with mild and severe edema with or without preoperative conservative treatment including compression. Under local anesthesia for adult patients (general anesthesia for children), after making short incisions on the medial aspects (totally two or more incisions, each 3 cm in length), the lymphatics and subdermal venules (each 0.5 mm in diameter) are explored using a loupe or operating microscope. The affected lymphatics are often dilated or sclerotic. Dye staining is not always a good indicator for finding lymphatics. When no suitable lymphatics are found in one site, incisions are made in other portions of the leg and foot dorsum. The subdermal venules, which exist anywhere beneath the dermis, can be usually detected adjacent to the lymphatics. Regarding the selection of these channels, lymphatics with strong drainage function, which are easily detected after transecting them under an operating microscope, should be selected to establish powerful lymphovenous shunting. Small subdermal venules of 0.5 mm caliber size are most suitable for joining with the lymphatics, because larger cutaneous veins may have higher intravascular pressure than that of the lymphatics. Larger dilated lymphatics greater than 0.5 mm, which are sometimes detected in either the superficial or the deep adipose layer, are anastomosed to the small branches of the main cutaneous vein. Without a vascular clamp, end-to-end lymphaticovenular anastomoses of the same size are carried out using 50-μm needle sutures (with 12–0 nylon) with a fine needle holder under high magnification (× 20–30 magnifications; ▶ Fig. 24.1, ▶ Fig. 24.2). Although this operation can be completed within 3 hours, some patients with an irradiated bladder need catheter urination. Postoperatively, a low-pressure bandage and a vascular dilating drug (prostaglandin E1) are applied and the patients are allowed to walk freely. Use of elastic stockings is started 2 weeks later for at least half a year.2,3
• Combined surgical treatment including lymph vessel transplantation: Since 2004, for severe limb lymphedema against LVA, we have been performing combined surgery including lymphatic vessel with functioning smooth muscle cells from the normal donors, multiple LVA, and liposuction, simultaneously or consequently.7 In the lymphatic transplantation method, lymphatic vessels having drainage functions of the lateral chest and the first web space are collected with nutrient blood vessels. It is divided into multiple pieces, transferred into the affected portions and limbs, and anastomosed with a fain recipient vessel (muscle penetrating branch), which nourishes the skin of the affected limb. If possible, LVA both inside and outside of the flap is established. Loss of drainage function of lymphatic vessel can be reconstructed with this method. This method has been followed in about 200 cases resisted to multiple LVA up to now; 10% did not required compression therapy (functional recovery) and 50% showed improvement. As we are currently popularizing this combined technique overseas, it will be a mainstream in the future (▶ Video 24.1).
Related posts:
 General Wound Preparation and Timing
General Wound Preparation and Timing
 The Pertinence of the Reconstructive Ladder and the Reconstructive Elevator
The Pertinence of the Reconstructive Ladder and the Reconstructive Elevator
 Supermicrosurgery Approach to the Lower Limb
Supermicrosurgery Approach to the Lower Limb
 Lower Limb Vascularized Composite Allotransplantation
Lower Limb Vascularized Composite Allotransplantation
 Using the Flap and Angiosome Concepts to Optimize Functional Lower Leg and Foot Amputations
Using the Flap and Angiosome Concepts to Optimize Functional Lower Leg and Foot Amputations
 Procurement of Thin Flaps as Indicated in the Lower Extremity
Procurement of Thin Flaps as Indicated in the Lower Extremity
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


