Embryology
Genetic sex is determined at fertilization, either XX or XY. For the first 6 weeks of development, gender is not distinguishable, and this is known as the indifferent period. Characteristic external genitalia begin forming about the ninth week of gestation.
Sexual differentiation of the internal and external female genitalia requires no active intervention or ovarian activity; it is considered the default pathway. However, androgen production by the Leydig cells and Mullerian inhibiting hormone (MIH) production by the Sertoli cells are required for the development of the male external genitalia.
The internal genitalia can only develop into one gender and are termed “unipotent.” In the male, the Wolffian ducts develop from the mesonephric ducts, and in the female, the Mullerian ducts develop from the paramesonephric ducts. In the male, MIH and androgens prevent development of female internal genitalia. In addition, androgens actively maintain the Wolffian ducts, whereas MIH induces the regression of the Mullerian ducts. In the female, Wolffian ducts regress in the absence of androgens ( Fig. 4.1 ).
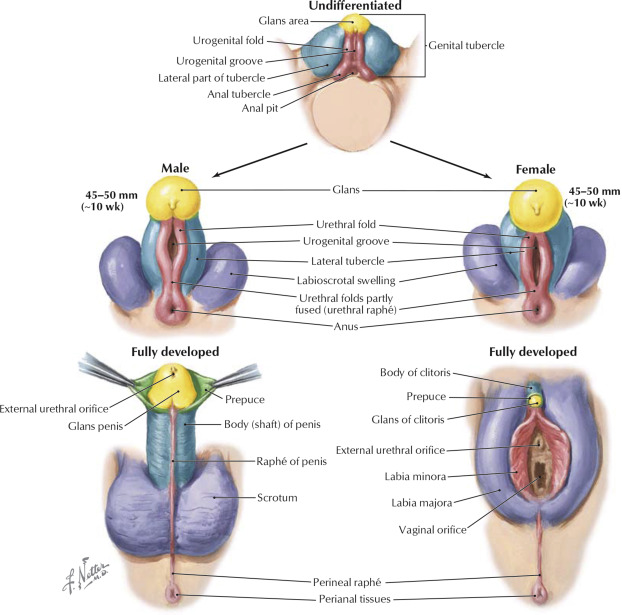
External genitalia have the potential to be either male or female and are termed “bipotential.” In order to develop male external genitalia, androgens are required. In both sexes, in about the fourth week of development, the genital tubercle elongates to form the phallus. In a developing male, androgens induce the fusion of the urethral folds to form the urethra. In addition, the genital tubercle enlarges to form the glans penis, and midline fusion of the genital swellings results in formation of the scrotum. In the female, the urethral folds and genital swellings remain separate and form the labia minora and majora. The genital tubercle forms the clitoris.
From the author’s perspective, in constructing the appropriate physical morphology, the relevant homologous structures are used to create “like-with-like.” This philosophy forms the foundation on which he has developed his surgical techniques.
Goals of surgical therapy
Congruent Genitalia
As described in the Standards of Care (SOC), the overarching treatment goal for transgender individuals is to maximize health, well-being, and fulfillment ( Figs. 4.2 and 4.3 ). Toward this end, gender confirmation surgery can provide the appropriate physical morphology and alleviate the extreme psychological discomfort that many patients experience. Furthermore, as discussed by Meyer in 2001 and Cohen-Kettenis and Kuiper in 1984, adjusting the mind to the body is not an effective treatment, while adjusting the body to the mind is the best way to assist severely gender dysphoric persons.


Congruent genitalia can allow an individual to experience harmony between one’s body and self-identity, appear nude in social situations without violating taboos (ie, bathrooms, locker rooms, physician offices), and, in some states, have legal identification concordant with their physical appearance.
Surgical goals for transwomen
Vaginoplasty
A successful surgical result involves the creation of a natural-appearing vagina and mons pubis that are sensate and functional, including removal of the stigmatizing scrotum, creation of feminine-appearing labia majora and minora, construction of a sensate neoclitoris, and development of adequate vaginal depth and introital width for intercourse. Additional desirable qualities include a smooth, graded, and contiguous appearance to the labia majora, a moist appearance to the labia minora simulating the vestibular lining in natal females, clitoral hooding, and lubrication for intercourse ( Box 4.1 , Fig. 4.4 ).
- •
Removal of the scrotum
- •
Feminine-appearing labia majora
- ○
Smooth, graded, and contiguous appearance
- ○
- •
Feminine-appearing labia minora
- ○
Moist appearance simulating the vestibular lining
- ○
- •
Sensate neoclitoris with clitoral hood
- •
Adequate vaginal depth and width for intercourse

Ancillary procedures
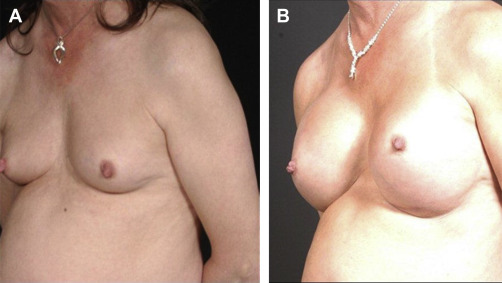
Aside from genital reconstruction, breast augmentation , thyroid chondroplasty (“tracheal shave”), facial feminization , and body contouring offer additional procedures designed to feminize one’s appearance ( Figs. 4.5 and 4.6 ).

Surgical goals for transmen
Chest surgery
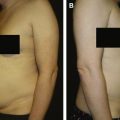
This procedure, commonly performed before genital surgery, involves bilateral subcutaneous mastectomies, liposuction of the chest, and repositioning and resizing of the nipple-areola complex, when necessary. Several different techniques are used, and the choice of technique depends on the volume of breast parenchyma, degree of breast ptosis, position and size of the nipple-areola complex, and degree of skin elasticity ( Box 4.2 , Fig. 4.7 ).
Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


