Abstract
In order to develop a safe surgical practice, the dermatologic surgeon should have a thorough knowledge of the etiology, management, and prevention of surgical complications. In this chapter, we will begin by reviewing several surgical complications. Then a diversity of techniques for scar revision will be discussed, including what type of scars each technique is best utilized for, as well as how to perform the different procedures described.
Keywords
scar revision, hematoma, infection, Z-plasty, W-plasty, geometric broken line closure, resurfacing
Having a thorough knowledge of common dermatologic surgery complications is essential for physicians to develop a safe surgical practice. Overall, the incidence of complications in dermatologic surgery is very low. However, complications are to be expected, particularly in practices with a high volume of dermatologic surgical procedures. Therefore it is critical the physician know how to manage complications.
Before performing a surgical procedure, an experienced dermatologic surgeon should visualize the steps of the procedure from start to finish, including the management of potential side effects. By doing this, many complications can be prevented. For example, if a patient is on anticoagulant medication, the physician will recognize that the patient is at a higher risk for hematoma formation. Therefore the surgeon will take extra precautions to ensure adequate management of hemostasis, such as having the medical assistant hold firm pressure for 8–10 minutes following suture closure.
In this section the most common surgical complications will be reviewed, including their etiology, management, and prevention. Of note, specific complications associated with various surgical flaps are discussed throughout this textbook.
Hemorrhage
Postoperative bleeding is one of the most common complications of cutaneous surgery. A variety of factors contribute to postoperative hemorrhage, including medications, inadequate intraoperative hemostasis, suboptimal wound closure that fails to obliterate tissue dead space, poorly controlled hypertension, and patients overexerting themselves after surgery.
Although achieving adequate hemostasis during the surgical procedure is critical for preventing postoperative bleeding, the prevention of postoperative hemorrhage is primarily managed preoperatively and postoperatively. For example, when patients are scheduled for their surgical procedure, they should be provided with instructions regarding how to prepare for surgery, such as whether they should withhold any medications, vitamins, and/or supplements. Of note, certain over-the-counter vitamins and supplements, such as vitamin D, vitamin E, fish oils, garlic, ginseng, and St. John’s wort, increase the risk of bleeding. Therefore many dermatologic surgeons recommend patients withhold these vitamins and supplements 2–3 weeks prior to the procedure. In addition, it is important for the physician to be familiar with the current guidelines for withholding anticoagulants and platelet inhibitors.
Among dermatologists there is a general consensus that continuation of anticoagulants, such as warfarin, is associated with a very low risk of surgical complications. Therefore continuing anticoagulant therapy is strongly favored, since a postoperative bleed is easier to manage and has a significantly lower morbidity/mortality risk compared with a stroke or embolus from discontinuation of the medication. There may be certain instances in which reduction or cessation of anticoagulation therapy is warranted. In such instances, this decision is best made on an individual basis. Moreover, the physician prescribing and managing the patient’s anticoagulant therapy should be explicitly involved in the decision on whether to hold or continue the medication.
Following the procedure, a good pressure dressing should be placed. If the patient is on aspirin, warfarin, or other anticoagulant therapy, firm pressure should be held for 8–10 minutes before placing the surgical dressing. The pressure dressing should remain in place for 24 hours. Patients should be instructed on how to properly change the pressure dressing and care for the wound. Likewise, they should be provided with instructions regarding how to manage a postoperative bleed, including holding firm, continuous pressure for 20 minutes. In addition, patients should be advised to avoid vigorous activities (e.g., exercise, bending over, heavy lifting, pushing, pulling) for several weeks following surgery, since such activities can increase the risk of postoperative bleeding and wound dehiscence.
Early, active postoperative bleeding can often be successfully managed with direct pressure to the wound. First, any saturated, wet bandages should be discarded. A dry gauze bandage should then be applied to the wound and held in place with continuous, firm pressure for 20 minutes. If bleeding continues, patients should be advised to call the surgeon and return to the office or local emergency room promptly. Excessive postoperative bleeding and expanding hematomas are primarily treated via the following procedure: (1) partial or complete opening of the surgical wound, (2) identification of the culprit blood vessel(s), (3) hemostasis with electrosurgery and/or suture ligation, (4) possible irrigation and lavage of the surgical wound with sterile sodium chloride (if a hematoma needs to be evacuated), and (5) reclosure of the wound or allowing the wound to heal via second intention. The latter option is considered if the wound is contaminated or if the patient is at a high risk for additional postoperative bleeding.
For patients who present a few days postprocedure with a stable hematoma, one can consider monitoring the area versus evacuating the hematoma. Small, stable hematomas with no necrosis of the overlying skin can often be managed with observation. If the area is extremely tender or if the overlying skin exhibits features worrisome for necrosis, the hematoma should be evacuated. This can often be accomplished under local anesthesia by making a small incision and inserting a cannula attached to a syringe to evacuate the hematoma. To help break up the blood clot, one can irrigate the wound with normal saline and aspirate the fluid using the syringe. If the cannula/syringe technique is unsuccessful, then the sutures should be removed to enable adequate evacuation of the hematoma. The wound can subsequently be resutured or allowed to heal via second intention.
Infection
The risk of surgical site infection (SSI) following dermatologic surgery is usually less than 5%. Staphylococcus aureus is the most common, isolated organism in SSIs. When reviewing postoperative care instructions, patients should be thoroughly educated regarding the signs and symptoms of SSI, which include an increase in erythema, pain, warmth, and/or edema at the wound site. These signs and symptoms typically present 4–6 days postoperatively. Patients should be strongly encouraged to contact the clinic if they have any questions/concerns regarding the surgical wound.
Usually SSI associated with dermatologic surgery can be managed on an outpatient basis. If possible, exudate from the surgical wound should be collected for bacterial culture and sensitivity. Patients should be started on broad-spectrum antibiotics with close follow-up care to monitor clinical response. The potential sequelae of wound infection include pain, prolonged healing, and altered aesthetic outcome.
Infection control and prevention includes thoroughly reviewing the patient’s medical history and medication list to identify patients at a higher risk of SSI. Risk factors include diabetes, poor nutrition, and immune suppression (e.g., transplant patients, patients undergoing chemotherapy, HIV). For patients undergoing dermatologic procedures around the lips, it is important to inquire about a history of herpes infection. If patients have a history of cold sores, they should be prescribed prophylactic oral antiviral therapy with acyclovir or a related medication.
Another important aspect of infection control/prevention is strict surgical aseptic protocol by the surgical team.
The use of oral postoperative antibiotics following dermatologic procedures remains a controversial topic. Surgical sites at higher risk for SSI include the lower extremities, genitals, ear, nose, eyelids, and lips. Thus when surgery is performed at these locations, the dermatologic surgeon may opt to prescribe a short 5–7 day course of oral antibiotics.
Wound Dehiscence
Wound dehiscence is the unintentional separation and reopening of the wound following surgery. This occurs when there is excessive tension and strain on the wound edges. For instance, inadequate undermining during surgery can result in increased tension on the wound edges. Surgical wounds located on highly mobile and high-tension areas, such as the hands, back, shoulders, or lower extremities, are at a higher risk for wound dehiscence. Other risk factors include tobacco use, previous scarring or radiation to the surgical site, and chronic use of topical or systemic corticosteroids. Poor patient compliance regarding wound care instructions, such as failure to avoid exertional activities for 1–2 weeks following surgery, can result in wound dehiscence. In addition, blunt trauma to the surgical site following suture removal can result in wound dehiscence, since scar tissue is weaker than surrounding, unaffected tissue, especially during the first 4 weeks postprocedure. At the time of suture removal, Steri-Strips can be placed to help decrease tension on the surgical wounds.
The management of wound dehiscence includes resuturing the wound edges versus allowing small dehiscent areas to heal by second intention. One should consider reclosure of the wound with sutures if dehiscence occurs within a few days following the initial procedure, if there is no evidence of infection, or if there is a deep dehiscent area. Oral antibiotics should be started if there are signs/symptoms of infection. Close follow-up care is critical to ensure assessment of the healing process and aesthetic outcome.
Eyelid Swelling/Lymphedema
Prolonged swelling of the lower eyelids due to lymphedema is a potential complication of procedures involving the lower eyelid and upper cheek. Lymphatic drainage of the eyelid primarily occurs laterally and inferiorly along the cheek. Excess wound closure tension, particularly on the lateral cheek and lower eyelid, results in temporary compression of the eyelid lymphatics, thereby impairing drainage of lymph fluid. In addition, lymphedema can result from disruption of the lymphatic system during tissue undermining. Therefore the surgeon can minimize the risk of lymphedema by doing minimal undermining in the lower eyelid region. To avoid exacerbating lymphedema, patients should be advised to avoid rubbing the lower eyelid and cheek, as this friction and blunt trauma can result in additional disruption of the eyelid lymphatic drainage system. Usually lymphedema will gradually resolve with time. However, if there has been extensive disruption of the lymphatics, the lymphedema may be chronic and persistent.
Ectropion
Ectropion is a condition in which the lower eyelid is turned outward, thereby leaving the inner eyelid surface exposed, resulting in irritation to the cornea. In addition, the lower eyelid eversion can result in an inability to fully close the eye. The most common cause of ectropion is wound closure tension vectors that result in downward displacement and eversion of the lower eyelid. Postoperative edema can cause temporary ectropion that gradually resolves with the swelling. In addition, injury to the branch of the facial nerve (CN VII) that innervates the orbicularis oculi muscle, which functions to close the eye, can result in ectropion.
To reduce the risk of ectropion, the surgeon should avoid placing sutures that result in wound tension creating downward pull on the lower eyelid. Therefore the orientation of the key sutures to close the primary defect is critical, since it determines the tension vector on the wound edges. Ideally the key sutures should be placed perpendicular to the lower eyelid margin. By doing this, the surgeon can avoid downward pull and eversion of the lower eyelid.
Patients with ectropion should be advised to use over-the-counter, lubricating eye drops several times a day to reduce dryness and irritation of the cornea. Options for surgical management of ectropion include canthopexy versus a full-thickness skin graft.
Motor Nerve Deficits
Prior to performing any procedure, the surgeon should consider if there are any major motor nerves within the surgical zone that could possibly be damaged. Before obtaining written, informed consent from the patient, the surgeon must educate the patient regarding potential complications, including possible nerve damage. To avoid nerve damage, it is critical for the surgeon to have a detailed knowledge of the anatomy of the head and neck and pay close attention to the tissue plane of undermining. Refer to the Chapter 1 discussion on anatomy for a detailed explanation of the danger zones and proper undermining plane for the various regions on the face.
Scars
Scar formation is an inevitable consequence of cutaneous surgery. The primary goals of surgical repair include (1) preserving/restoring function of anatomical units/subunits; (2) creating a minimally visible, fine-line scar; and (3) preserving/maintaining symmetry and contour of anatomical units. From the patient’s perspective, one of the most significant factors determining the success of a cutaneous surgical procedure is the aesthetic appearance of the final scar. Therefore the surgeon should be familiar with various techniques to improve the appearance of the final surgical scar. This includes surgical techniques during the initial repair, as well as techniques for revising the scar.
There are several ways to classify scars. For instance, scars can be classified by their underlying cause, such as surgical scars, acne scars (which can be further subclassified into depressed scars, including boxcar, icepick, and rolling scars), raised scars (which are subclassified into hypertrophic and keloid scars), and scars secondary to trauma (e.g., lacerations, abrasions, thermal burns, chemical burns). Another means to classify scars is to categorize them as being either raised or depressed. The International Advisory Panel on Scar Management classifies scars via the following categories: mature, immature, linear hypertrophic, widespread hypertrophic, minor keloid, and major keloid.
When evaluating and describing scars, one should note the following features: thickness, visibility, erythema, contour, texture, vascularity, hypopigmentation or hyperpigmentation, symmetry to contralateral side, and relation to relaxed skin tension lines (RSTLs). In addition, it is important to note whether the patient is experiencing functional impairment of the involved anatomical unit/subunits, such as inability to fully close or open the eyes, difficulty breathing through the nose due to nasal valve collapse, and inability to open or close the mouth. Successful scar revision is usually optimized with a combination approach to address these different features.
Scar Revision
The main goals of scar revision are to make scars less noticeable and more aesthetically acceptable. Prior to performing scar revision, the surgeon should discuss the realistic, expected outcomes and manage patient expectations.
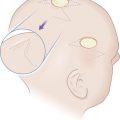
Improving surgical outcomes and minimizing the visibility of scars entails the surgeon having a sound understanding of anatomical form, the function of anatomical subunits, and an appreciation for free margins. When assessing a scar, just as when assessing a surgical wound, the surgeon should note which cosmetic units and subunits the defect involves, have a good understanding of tissue recruitment and tension vectors, and determine the direction of the RSTLs. Meticulous surgical technique always plays a key role in surgical aesthetic outcomes. Important features of meticulous surgical technique include minimizing wound tension, good reapproximation of fresh wound edges, and wound edge eversion. Precise surgical technique is key, as failure to properly align wound edges will result in an irregular scar ( Fig. 18.1 ).