Abstract
Skin cancers commonly occur on the forehead and temple and many require surgical removal. Skin and soft tissue defects resulting from skin cancer removal from these sites range from simple to challenging in terms of size, depth, and reconstructive options. Fundamental principles including complete tumor removal and an understanding of cosmetic units, relaxed skin tension lines, and respect for anatomic free margins are key in optimizing outcome. In the following chapter, these principles along with relevant anatomy and surgical technique will be reviewed leading to design and execution of linear, flap, and graft repair for defects involving the forehead and temple.
Keywords
forehead wound, reconstructive surgery, advancement flap, rotation flap, transposition flap, skin graft
Successful treatment of the skin cancer patient revolves around three goals: (1) tumor-free surgical margins; (2) preservation of function; and (3) restoration and optimization of cosmesis. Before conceptualizing any repair, the surgeon must keep in mind that the primary goal of the oncologic surgeon is achievement of a tumor-free plane. Residual tumor will lead to recurrence, which can be devastating functionally and cosmetically, and potentially life threatening with aggressive tumors. One must understand tumor biology and relevant anatomy in order to be successful in this endeavor. From an aesthetic perspective, reconstructions planned according to the cosmetic unit principle provide optimal cosmesis.
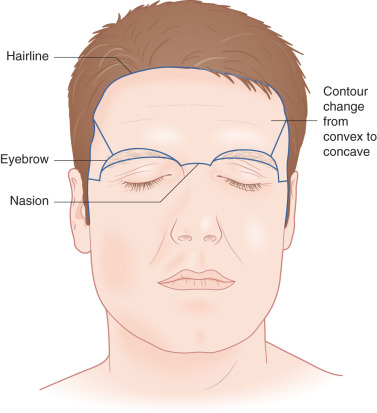
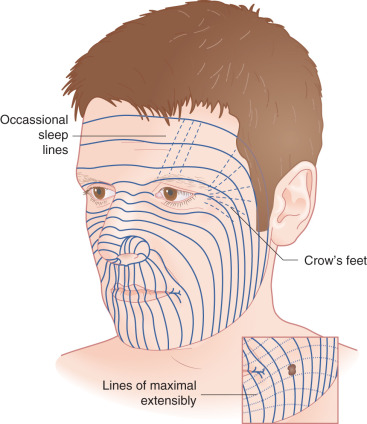
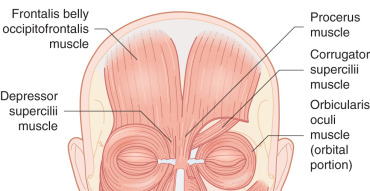
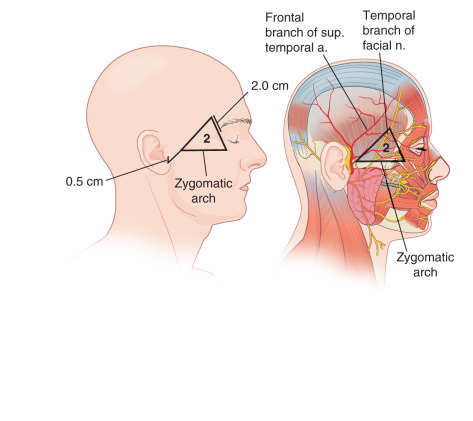
The forehead, which includes the temple region, is defined superiorly and laterally by the natural anterior hairline and inferiorly by the zygomatic arch, eyebrows, and nasal root. It may be subdivided into five subunits: the central forehead, which is contiguous with the scalp; the bilateral temples; and the hair-bearing eyebrows ( Fig. 11.1 ). Relaxed-skin tension lines (RSTLs) run horizontally in the central forehead, perpendicular to the underlying frontalis musculature, and curve laterally as the temple is approached ( Fig. 11.2 ). Convex centrally, the lateral subunit of the temple is relatively concave. Composed of moderately sebaceous skin, the central forehead is relatively immobile, with adherence to the underlying frontalis muscles. The temple subunit is more mobile, as it is loosely adherent to the underlying temporal fascia. The paired frontalis muscles insert into the inferior musculature and the brow without muscle directly midline. Inferiorly, the procerus muscle acts centrally, with bilateral corrugator supercilii muscles, and more laterally the superior aspects of orbicular oculi ( Fig. 11.3 ). The superficial musculoaponeurotic system (SMAS), which underlies the dermis and subcutaneous tissue superiorly, is composed of the galea aponeurotica of the scalp, which invests the frontalis muscle and orbicularis oculi. Laterally, the galea is contiguous with temporoparietal fascia. In the temporal region, the superficial temporal fascia lies just beneath the subcutaneous tissue and is contiguous with the galea superiorly, the frontalis muscle, and the SMAS. Deep to this layer is the innominate fascia. Concern in this region must be taken for preservation of the temporal branch of the facial nerve, which generally runs just beneath the superficial temporal fascia within the SMAS creating a relative “danger zone,” though some consider this branch to course deeper in the innominate fascia. This region is generally defined inferiorly by a line drawn from the earlobe to the lateral brow and superiorly by a line drawn from the tragus to the lateral aspect of the highest RSTL on the forehead, with the nerve being most superficial and at risk as it crosses the midzygomatic arch ( Fig. 11.4 ).
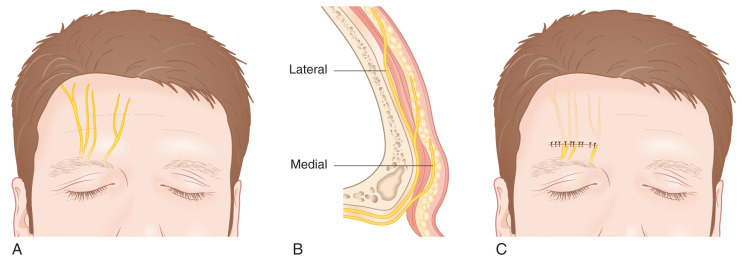
Vascular supply to the majority of the forehead is supplied by the dorsal nasal artery, supratrochlear artery, and supraorbital artery, all branches of the internal carotid artery. The supratrochlear artery, which is most medial, is the axial artery for the paramedian forehead flap. Laterally, the temple region is supplied by the superficial temporal artery, which arises from the external carotid artery ( Fig. 11.5 ). This artery runs within and then above the SMAS layers of the lateral forehead. Generally, two undermining planes may be defined on the forehead—above the frontalis muscle and below the muscle and deep fascia. This latter plane provides a relatively bloodless plane but can result in transection of the major vessels and requires repair of the frontalis muscle. Sensory innervation mirrors the vasculature medially and arises from the supratrochlear and supraorbital branches of the ophthalmic division of the trigeminal nerve ( Fig. 11.6 ). These nerves divide into four to six terminal branches collectively and may have variable anatomy, but notably these nerves quickly penetrate the muscle and enter the superficial subcutaneous plane after leaving their foramens. As a result, horizontal closure in this area may result in a fan-shaped area of numbness superior to the closure that is usually temporary. Laterally the temple receives sensory innervation from the zygomaticotemporal nerve, a branch of the maxillary division of the trigeminal nerve. Motor innervation is provided predominantly by the temporal branch of the facial nerve. Contraction of the frontalis muscle causes brow elevation, and denervation results in brow ptosis. The paired corrugator supercilii muscles are also innervated by the temporal branch of the facial nerve and act to pull the brow medially and downward while the central procerus muscle is innervated by the zygomatic branch of the facial nerve and acts to depress the brow. Laterally the paired orbicular oculi muscles are innervated by the temporal branch of the facial nerve and act to close the eyes.

As in the case of surgical defects in any location, various repairs may be considered on the forehead. Generally a poor match for skin grafts, secondary intention, primary linear closure, M-plasty, advancement flaps including rotation flaps, and transposition flaps may all be considered in this subunit. Which type of repair is optimal depends on the size and location of the defect, as well as the patient’s individual anatomy. Maintenance of brow position is of utmost importance with respect to cosmesis, and consideration of tension placed on the eyelid must be observed more laterally in the temple region.
Reconstructive Principles
Secondary Intention
Surgical defects on the concave aspect of the lateral temple generally heal significantly better than the convex central forehead when allowed to granulate. Wound healing by secondary intention results in flat or slightly depressed, hypopigmented scars. The risk of hypertrophic scarring and brow or eyelid distortion is rare if the defect is not too large. Additionally, healing by secondary intention may prolong wound care, and patients should be seen at regular intervals to ensure proper wound care is being performed. Biologic dressings are an option for forehead closure to stimulate granulation tissue, especially if the defect has areas of exposed bone ( Fig. 11.7 ). Currently the authors favor porcine xenograft sutured with 5-0 or 6-0 fast absorbing gut in these cases.

Primary Linear Closure
Horizontal and vertical primary linear closures are the mainstays for reconstruction of the forehead. Vertical closures are especially well suited to prevent elevation of the brow, and can be hidden in RSTLs created by the procerus and corrugator supercilii for centrally based forehead defects. In addition, vertical closure may prevent the numbness that can be temporarily produced with horizontal closures. Horizontal closures, on the other hand, are significantly masked in the RSTLs created by the frontalis muscle ( Fig. 11.8 ). In general, forehead defects measuring up to 1.0 cm in diameter may be closed in a horizontal fashion with minimal risk of permanent change in brow position, depending upon several anatomical factors such as skin laxity, brow ptosis, eyelid redundancy, and the location of the defect. The higher the location of the defect on the forehead, the less likely brow distortion is to occur. The brow may elevate when the wound edges are approximated during reconstruction of even these smaller defects; however, this elevation is usually temporary. Typically, the brow will return to its normal or near-normal position 1 to 2 months following surgery. When considering whether vertical or horizontal repair is optimal, consideration should be given to use of RSTLs, the closure of which will place minimal tension on the wound, and brow placement ( Fig. 11.9 ). In the lateral region of the temple, radial orientation of the orbicularis oculi muscle should prompt consideration for closure in a radial direction ( Fig. 11.10 ). Finally, modification of the standard elliptical closure using an M-plasty is particularly useful in the temple to avoid the lateral canthus ( Fig. 11.11 ; Box 11.1 ).