A detailed understanding of nasal anatomy is essential when undertaking rhinoplasty surgery. This article describes the nasal anatomy, careful study of which makes for a more confident, prepared practitioner.
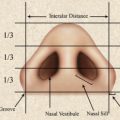
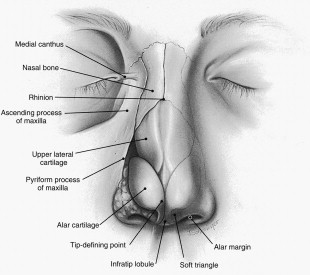
Assessing the external nose requires an understanding of the anatomic components that contribute to its normal topographic features. Structures that influence the external appearance include the skin, which varies in thickness, and the underlying bony/cartilaginous skeletal framework. Because skin thickness is greatest at areas of skeletal narrowness, the external appearance of the nose from the frontal view is one of a soft, gentle curve emanating from the medial brows and extending to the tip-defining points (dorsal esthetic line) ( Fig. 1 ). The lobule can be defined as an area including the tip of the nose and bounded by a line connecting the upper edge of the nostrils, the supratip breakpoint, and the anterior half of the lateral alar wall. The lobule is subdivided into the tip, supratip, and infratip lobule. On lateral view, one should be aware of the marked differences in the thickness of the soft tissue ( Fig. 2 ).
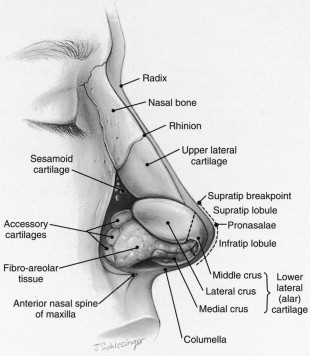
The internal structure most frequently responsible for the prominence of the lateral tip-defining point or pronasalae is the cephalic edge of the domal segment of the middle crus. On lateral view, the tip of the nose is the apex of the lobule and ideally the most defined element on the profile. In non-Caucasian, however, the tip tends to lack definition. The infratip lobule is between the tip and the apex of the nostrils. The configuration of the infratip lobule depends on the shape, size, and angulation of the medial and middle crura of the alar cartilage (see Fig. 2 ). The supratip lobule lies between the pronasalae and the supratip breakpoint. The nasolabial angle is defined as the angle formed by a line drawn from the anterior to the posterior nostril apices and intersects with the vertical facial plane. It determines the amount of cephalic rotation of the tip.
In an esthetically pleasing nose, the columella projects as a gentle curve below the alar margin as seen on lateral view. In the non-Caucasian nose, however, a common variation is for the ala to overhang the columella posteriorly. The columella and infratip lobule projection are influenced by the configuration of the medial and middle crura. Because of the thin, adherent skin, asymmetries or prominences in these structures are easily visible in external configuration. In addition, projections of the caudal edge of the septum can produce a prominence of the columella also.
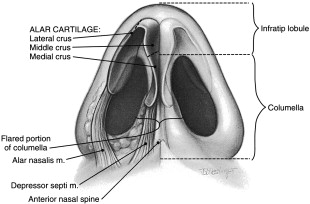
On base view ( Fig. 3 ), the flaring of the caudal edges of the medial and middle crura is noted. The degree of flare plus the lateral curve of the medial crural footplates determine the width of the columella and infratip lobule. Columellar deviations and asymmetries are frequently caused by deflections in the caudal septum. Medially, the relationship should be noted of the anterior nasal spine to the depressor septi muscle, which is paired and inserts into the medial crural foot plates. Laterally, the alar part of the nasalis muscle should be noted.
Soft-tissue covering of the nose
Skin
Skin thickness is one of the most important features to assess preoperatively in planning rhinoplasty. The skin tends to be thinner and more mobile in the upper half of the nose and thicker and more adherent distally. In dissections reported by Lessard and Daniel, average skin thickness was noted to be greatest at the nasofrontal groove (1.25 mm) and least at the rhinion (0.6 mm). There are usually more sebaceous glands in the lower half of the nose, causing an oiliness and thickness in the skin that may limit topographic definition, sometimes obscuring entirely the underlying framework and the natural esthetic lines normally visible, particularly in the non-Caucasian nose, which may have a larger subcutaneous dense fibrofatty layer than the Caucasian nose. Some of the nasal changes seen with aging (ie, tip droop, nasal lengthening) may be caused by changes in skin character. The skin is usually thinner along the alar margin and in the columella, where the configuration of the alar cartilages may be visualized through a thin skin cover. The skin-to-skin approximations in the soft triangle area at the nostril apex makes it extremely vulnerable to notching and irregularities due to scarring when intranasal incisions violate this delicate area.
Subcutaneous Layer
The soft tissue intervening between the skin and the osteocartilaginous skeleton is made up of four layers. They are the superficial fatty panniculus, the fibromuscular layer, the deep fatty layer and the periosteum or perichondrium . The fibromuscular layer includes the nasal subcutaneous muscular aponeurotic system (SMAS). The nasal SMAS is a continuation of the superficial muscular aponeurotic system, which covers the entire face, interconnecting the facial musculature, the galealfrontalis layer, and the platysma. Ignorance of the importance of this level or inadvertent surgical or traumatic division of the superficial muscular aponeurotic system (SMAS) leads to its bilateral retraction. This retraction exposes the deeper skeletal components to possible adherence through scar tissue to the superficial fatty layer, which is directly connected to the dermis. The major superficial blood vessels and motor nerves run within the deep fatty layer. Just beneath it and superficial to the periosteum and perichondrium is the proper plane of dissection, similar to the areolar layer beneath the galea aponeurotica in the scalp.
Muscles
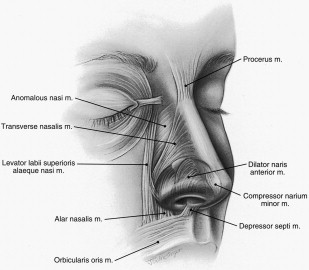
Griesman subdivided the nasal muscles into four groups. Letourneau and Daniel substantiated these findings in 30 fresh cadaver dissections ( Fig. 4 ). The elevator muscles, which shorten the nose and dilate the nostrils, include (1) the procerus, (2) the levator labii superioris alaeque nasi, and (3) the anomalous nasi. The depressor muscles, which lengthen the nose and dilate the nostrils, include (4) the alar portion of the nasalis muscle (dilator naris posterior) and (5) the depressor septi. The minor dilator muscle is the (6) dilator naris anterior. The compressor muscles, which lengthen the nose and narrow the nostrils, include (7) the transverse portion of the nasalis and (8) the compressor narium minor. An in-depth discussion of these muscles can be found in articles by Griesman and Letourneau and Danie1. All the muscles are innervated by the zygomaticotemporal division of the facial nerve.
External blood supply
The superficial arterial supply to the external structures of the nose is derived from the internal carotid artery (through the ophthalmic) and external carotid artery (through the facial and internal maxillary) ( Fig. 5 ). The lateral surface of the caudal nose is supplied by the lateral nasal branch from the angular artery, which is the continuation of the facial artery. This branch anastomoses with its pair from the opposite side across the dorsum of the nose. Herbert referred to the angular artery as an alar branch of the superior labial artery. He noted that it passed deep in the groove between the ala and the cheek and lay buried in the levator labii superioris alaeque nasi muscle. It tended to follow closely the margin of the pyriform aperture. Sequentially it gives off between 7 and 12 short branches, which perforate the enveloping muscle and enter the subdermal plexus of the nostril and cheek. These branches provide a rich axial blood supply to subcutaneous based cheek and nasolabial flaps and the nasalis myocutaneous flap.
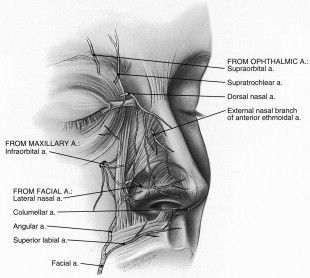
An external branch of the ophthalmic artery, the dorsal nasal artery, perforates the orbital septum above the medial canthal ligament and runs downward on the side of the nose to anastomose with the lateral nasal branch of the angular artery. It gives off a branch to the lacrimal sac. All of these vessels, which vary in size, are supplemented by twigs laterally from branches of the infraorbital artery. The dorsal nasal artery, which also can have communications with the supratrochlear and infraorbital arteries, forms an axial arterial network for the dorsal skin as described by Marchak and Toth. Injection studies quoted in their article show the rich anastomotic blood supply to the lateral skin of the nose, allowing elevation of this entire soft-tissue envelope on a narrow vascular pedicle.
Branches of the superior labial artery supply the nostril sill and the base of the columella. Consistently a substantial branch ascends in the columella just superficial to the medial crura (see Fig. 5 ). The columellar artery, which is often bifurcated, is cut with a transcolumellar incision used in the open rhinoplasty approach. The branches of the external nasal branch of the anterior ethmoidal artery along with the angular artery in the ala also contribute to the arterial supply to the nasal tip. The level of these vessels should be considered in open rhinoplasty to minimize compromise of the circulation to the nasal tip and columellar skin. It is also important to maintain dissection just superficial to the lateral crura of the alar cartilage to avoid injuring these lateral vessels. For the same reason, when performing open rhinoplasty, alar base excisions should always be limited to skin and superficial subcutaneous tissue.
The venous drainage of the external nose has the same-named veins, which accompany the arteries. These veins drain via the facial vein and the pterygoid plexus and through the ophthalmic veins into the cavernous sinus.
External blood supply
The superficial arterial supply to the external structures of the nose is derived from the internal carotid artery (through the ophthalmic) and external carotid artery (through the facial and internal maxillary) ( Fig. 5 ). The lateral surface of the caudal nose is supplied by the lateral nasal branch from the angular artery, which is the continuation of the facial artery. This branch anastomoses with its pair from the opposite side across the dorsum of the nose. Herbert referred to the angular artery as an alar branch of the superior labial artery. He noted that it passed deep in the groove between the ala and the cheek and lay buried in the levator labii superioris alaeque nasi muscle. It tended to follow closely the margin of the pyriform aperture. Sequentially it gives off between 7 and 12 short branches, which perforate the enveloping muscle and enter the subdermal plexus of the nostril and cheek. These branches provide a rich axial blood supply to subcutaneous based cheek and nasolabial flaps and the nasalis myocutaneous flap.
An external branch of the ophthalmic artery, the dorsal nasal artery, perforates the orbital septum above the medial canthal ligament and runs downward on the side of the nose to anastomose with the lateral nasal branch of the angular artery. It gives off a branch to the lacrimal sac. All of these vessels, which vary in size, are supplemented by twigs laterally from branches of the infraorbital artery. The dorsal nasal artery, which also can have communications with the supratrochlear and infraorbital arteries, forms an axial arterial network for the dorsal skin as described by Marchak and Toth. Injection studies quoted in their article show the rich anastomotic blood supply to the lateral skin of the nose, allowing elevation of this entire soft-tissue envelope on a narrow vascular pedicle.
Branches of the superior labial artery supply the nostril sill and the base of the columella. Consistently a substantial branch ascends in the columella just superficial to the medial crura (see Fig. 5 ). The columellar artery, which is often bifurcated, is cut with a transcolumellar incision used in the open rhinoplasty approach. The branches of the external nasal branch of the anterior ethmoidal artery along with the angular artery in the ala also contribute to the arterial supply to the nasal tip. The level of these vessels should be considered in open rhinoplasty to minimize compromise of the circulation to the nasal tip and columellar skin. It is also important to maintain dissection just superficial to the lateral crura of the alar cartilage to avoid injuring these lateral vessels. For the same reason, when performing open rhinoplasty, alar base excisions should always be limited to skin and superficial subcutaneous tissue.
The venous drainage of the external nose has the same-named veins, which accompany the arteries. These veins drain via the facial vein and the pterygoid plexus and through the ophthalmic veins into the cavernous sinus.
External sensory nerve supply
Sensibility to the external nose is mediated through branches of the ophthalmic and maxillary divisions of the fifth cranial nerve ( Fig. 6 ). Sensibility to the skin of the nose at the radix, the rhinion, and the cephalic portion of the nasal side walls is supplied by twigs from the supratrochlear and infratrochlear branches of the ophthalmic nerve. The external nasal branch of the anterior ethmoidal nerve, which emerges between the nasal bone and the upper lateral cartilage, accompanying the same-named artery, supplies the skin over the dorsum of the distal nose down to and including the tip of the nose. Injury to this nerve explains tip numbness commonly noted after rhinoplasty, as this branch is vulnerable during intercartilage or cartilage-splitting incisions. To minimize the chance of injury to this nerve, it is best to avoid deep endonasal incisions. Instead, the dissection should be maintained directly on the surface of the cartilage (deep to the fibromuscular layer and extension of the periosteum [SMAS]). Sensibility to the soft tissues on the side of the lower half of the nose is supplied through the infraorbital branches of the maxillary nerve, which also supplies portions of the columella and the lateral vestibule. Thus, an infraorbital block is important when relying on local anesthesia during rhinoplasty.
Caudal third of the nose
The lower third, or base, of the nose is made up of the lobule, columella, nostril floors, vestibules, alar bases, and alar side walls. It contains the paired alar cartilages and accessory cartilages and fibrous fatty connective tissue (see Figs. 1–3 ).
Alar Cartilage Morphology
The traditional concept of alar cartilage morphology was that of medial and lateral crura connected by an anatomic domal segment. To clarify the understanding of the surgical anatomy of the nasal tip, Sheen and Sheen introduced the concept of a middle crus , with its inferior limit at the columellar lobule junction and its superior limit at the junction of the medial extent of the lateral crus ( Figs. 7–9 ). Daniel’s observations place the domal segment in the most superior aspect of the middle crus. After Sheen’s original observation, the middle crus has also been referred to as the intermediate crus . The concept of a distinct and independent middle or intermediate crus has been challenged by another study, in which the term body or intercrural segment was applied. It is the authors’ opinion, however, that this structure is more than a connecting link between the medial and lateral crura. Its complex and variable structure is so important to the configuration of the nasal lobule that it deserves separate description and consideration. In this discussion, each alar cartilage is divided into 3 components: the medial , middle , and lateral crura .
Medial crus
The medial crus consists of two components: the footplate segment and the columellar segment . In most patients, angulation occurs in 2 planes: the angle of cephalic rotation , as noted on lateral view ( Fig. 10 ), and the angle of footplate divergence , as noted on base view (see Fig. 9 C). The effect of the configuration of the medial crus produced by these angles greatly influences the shape and prominence of the flared portion of the base of the columella (see Fig. 3 ). The footplate segment of the columella is influenced not only by its intrinsic shape but also by the posterior caudal edge of the cartilaginous septum, and by the amount of soft tissue in the base of the columella.
The columellar segment begins at the upper limit of the footplate segment and ends at the columellar lobule junction (columellar breakpoint), where it joins the middle crus. The length of the columellar segment varies. Elongated nostrils are due in part to vertically long columellar segments. Natvig and colleagues described three common anatomic variations of the medial crus in a cadaver study that were confirmed by others ( Fig. 11 ). The most common type is an asymmetric parallel (75%) ( Fig. 12 ). The other two types, the flared symmetric and the straight symmetric, occur about equally (12.5%). Although the skin is thin and the subcutaneous tissue is almost nonexistent laterally, the intervening soft tissue between the columellar segments of the medial crus frequently camouflages any asymmetries. In contrast, the absence of sufficient intervening soft tissue creates a bifid appearance of the columella. When performing an open rhinoplasty, it is important to elevate with the columellar skin flap at a depth to include all the intervening soft tissue. If this is not done, the inadvertent postoperative result could be an unplanned bifidity in the columella. When repositioning the columellar segments or resuturing them after separation to expose the caudal septum in open rhinoplasty, it is important to retain the natural flare of the caudal edges by placing any fixation sutures only at the cephalic borders.
From the lateral view, the most convex portion of the columellar lobular curve is termed the columella breakpoint (see Fig. 10 ). Its configuration is determined intrinsically by the shape of the junction of the columellar segment of the medial crus and the lobular segment of the middle crus. Acute angulations can produce an unattractive protrusion. The amount of protrusion of the columella (caudal projection) depends not only on the horizontal width of the columellar segment but also on the width of the membranous septum and the amount of protrusion of the caudal edge of the septal cartilage. Likewise, upward retraction depends on a deficiency of the same factors but most often is caused by retraction of the caudal septum because of trauma or congenital deformity or iatrogenically because of overresection of the edge of the caudal septum or failure to leave an adequate caudal septal strut during submucous resection of the septum.
Middle (intermediate) crus
The middle crus is made up of the lobular segment and the domal segment . The lobular segment of the middle crus tends to be the most variable and have the least correlation between the actual internal structural configuration and the external appearance. Its superficial expression is camouflaged by the thicker, overlying soft-tissue envelope.
The lobular segment tends to have the same variable configuration as described by Natvig and colleagues for the medial crus. Their description did not include the middle crus as a separate anatomic unit. Daniel and Letourneau, in describing their observations from open rhinoplasty, noted that in almost all cases the cephalic edges of the lobular segment were in close approximation but that the caudal edges diverged ( Fig. 13 ). Their length, configuration, and angulation determine the shape, height, and protrusion of the infratip lobule.
The domal segment is usually short and also frequently the most thin, delicate, and narrow portion of the entire alar cartilage arch. In contrast to Sheen’s earlier description, Daniel has described a medial genu at its connection with the lobular segment and a lateral genu at its junction with the lateral crus. The domal segment can vary in configuration ( Fig. 14 ). It may be concave, which is the least common. With the convex medial and lateral genu, this configuration produces a double-dome effect. It also can be smooth, which gives the tip of the nose a wide, boxy configuration. Varying degrees of convexity of the domal segment produce a more esthetic tip. The concave caudal edge of the domal segment frequently has a notched configuration (the domal notch), which is largely responsible for the facet of the soft triangle . The soft triangle is at the apex of the nostril, where dermis is in direct contact with dermis containing no intervening subcutaneous tissue. Because the caudal edge of the domal segment is so irregular and the cartilage itself is so delicate, great care must be taken in making infracartilaginous incisions to avoid injuring the cartilage edge or intruding into the soft triangle, where postoperative scarring may produce deformity in this delicate skin. The cephalic edges of the paired domal segments are frequently in close approximation or have minimal separation ( Fig. 15 ). The approximation of the domal segments also may extend to include the adjacent cephalic edge of the lateral crus. The cephalic edge usually slopes posteriorly from the high point of the domal segment in the normal esthetic nose to contribute to the supratip breakpoint (see Fig. 15 ). The paired domal defining points characteristically decrease at the most anterior projecting point along the domal segments. These defining points can be narrowed using sutures.