Surgery of Malignant Disease
3.2.1 Simple, Complex, and Oncoplastic Breast-Conserving Surgery
Aims and Methods
Development of breast-conserving surgery. Before 1950, breast cancer was treated by radical resection of the breast and pectoralis muscles, not least because the disease was often locally advanced. Following the Second World War, improved access to doctors and the concept of medical screening, aided by the introduction of mammography, led to ever earlier diagnosis of breast cancer. Epidemiologic data showed clearly that the patient’s long-term prognosis depended primarily on the tumor stage and especially the axillary node status at the time of the initial diagnosis and not on the surgical therapy. As a result, concepts of breast-conserving tumor resection (quadrantectomy) were developed, based on the pioneering work of Umberto Veronesi in Milan, Italy, and Bernard Fisher in Pittsburgh, United States and their colleagues; the scientific validity of these concepts has been confirmed by follow-up data over more than a quarter of a century. However, the level of acceptance of this technique varied from country to country. German surgeons rapidly recognized how important it was for women affected by breast cancer to avoid the mutilation of mastectomy and the consistent combination of oncological safety with patient-centered medicine was crucial for the establishment of breast surgery in the German surgical repertory.
Breast-conserving treatment today. More and more patients today are diagnosed and treated when their disease is at stage 1 or 2. For most of these patients, breast-conserving surgery (BCS) is the treatment of choice as small and unifocal carcinomas are suitable for this relatively simple operation. The aim of breast-conserving cancer therapy is oncologically acceptable resection of the tumor with an adequate margin of healthy tissue, tumor-free R status on histopathology, and a satisfactory postoperative cosmetic result.
Operation classification. Although the principles of all breast-conserving surgical techniques are similar, it is important for scientific and didactic reasons and not least for documentation to use uniform nomenclature for these operations. The classification given in Chapter 1.2.2 distinguishes between “simple,”“complex,” and “oncoplastic” operations. Simple BCS is histologically confirmed tumor excision (wide local excision to quadrantectomy) where the defect is covered by direct approximation alone, without mobilization of glandular tissue or skin flaps. Complex BCS is defined as histologically confirmed tumor excision (wide local excision to quadrantectomy) with intramammary reconstruction of the breast by subcutaneous or epifascial mobilization of glandular tissue to fill the defect, and with mobilization of a skin flap if necessary (< 25% mobilization). Oncoplastic BCS corresponds to complex BCS but with a mobilization volume greater than 25%. Periareolar de-epithelialization patterns to move the nipple are outside the limits of the various complex oncoplastic breast-conserving procedures (Chapter 3.2.2).
Indications and Contraindications
Indications
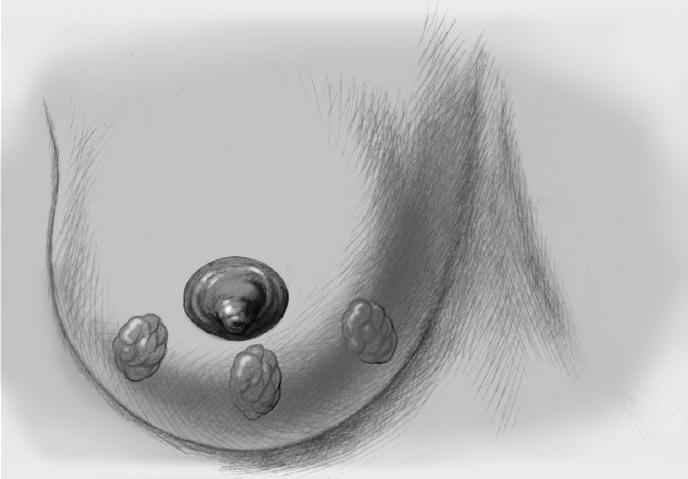
Breast surgery is indicated when a minimally invasive needle biopsy has provided a confirmed histological diagnosis of an invasive process or DCIS. Open biopsy was performed in the past but is no longer standard and is acceptable today only in rare, exceptional cases. If surgery is indicated, the primary decision is between mastectomy and a breast-conserving procedure. The criteria include the clinical tumor stage, especially tumor size, breast size and the relationship between tumor size and breast size, tumor location, risk situation, the patient’s wishes, and the possibility of postoperative radiotherapy. In the case of larger tumors, preoperative primary systemic (neoadjuvant) chemotherapy must also be considered. The classic indication for breast-conserving surgery is a small unifocal carcinoma. However, bifocal or multifocal tumors that do not extend beyond the segmental arrangement of the breast and are definitely confined to one quadrant are also suitable. Intraductal breast cancer without disseminated growth and a tumor size that is acceptable in relation to the size of the breast is a further potential indication for breast conservation.
Contraindications
Breast-conserving surgery is contraindicated when an extensive multifocal carcinoma does not allow adequate defect cover. Inflammatory and locally advanced tumors are nearly always contraindications to BCS and require mastectomy. Breast conservation is relatively contraindicated if postoperative adjuvant radiotherapy appears impossible as local recurrence rates are 15–30%. The essential requirement for esthetic breast conservation is oncologically safe resection relative to the volume and shape of the breast; this safety is the most important aspect in avoiding recurrence. Overall, resection margins of more than 1 mm are desirable with invasive carcinoma and more than 2 mm with DCIS. This is not always possible anatomically, for example, because of the posterior (muscle fascia) or anterior (skin) resection margin. In this case, the safety margins must be considered on an individual basis in a multidisciplinary conference.
If greater resections must be performed beyond the purely segmental anatomy, primary oncoplastic covering of the defect must be planned to ensure an esthetic outcome. Apart from the purely cosmetic aspect, this is important for follow-up as scarring in the operation area often renders diagnostic imaging more difficult.
Operation Risks and Informed Consent
As in nearly all breast surgery, the general operation risks are wound infection, secondary bleeding, hematoma, seroma, scarring, nerve injury, and impaired sensation in the skin and nipple–areola complex. In particular, the patient must be informed of the need for subsequent radiotherapy with possible retraction of the parenchyma. Intraoperative filling of the defect must be as complete as possible. Every patient must also be informed that further resection will be necessary if resection margins are narrow, or that mastectomy will be required if repeated secondary resection is necessary, extensive DCIS is present close to the tumor, and/or a multifocal carcinoma is found in the final specimen. The risk of local intramammary recurrence despite radiotherapy must also be discussed. Finally, the possibility of a poor cosmetic outcome must be addressed.
Operation Planning
All patients with histologically confirmed breast cancer should attend an interdisciplinary breast center to plan treatment and its timing.
Medical history, clinical examination (inspection and palpation), completion of histological diagnosis (if necessary), and diagnostic imaging
Imaging includes at least mammography and breast ultrasonography. MRI is indicated to exclude or confirm extensive multifocal breast cancer in the case of lobular carcinoma, or in the case of very dense breast tissue (grade 3 or 4).
Preoperative discussion of the patient by the breast team (breast surgeon, pathologist, and radiologist) and definitive planning of the extent of surgery, determination of the need for neoadjuvant systemic therapy
Discussion with the patient regarding the surgical procedure and potential risks
Patient’s consent to the procedure
The incision line is drawn with the patient standing or sitting up, either the day before or immediately prior to operation.
Thrombosis prophylaxis: low molecular weight heparin
Antibiotic prophylaxis: first or second generation cephalosporin
Easy to moderately difficult surgery; takes about 1 hour; surgeon and one assistant
Anesthesia and Positioning
Special Instruments
Breast set: dissecting scissors, electrocautery knife, electrocautery needle, skin hooks, Roux hooks
Procedure
Preparation
The patient should empty her bladder immediately before transport to the operating room.
The patient and the breast to be operated on are identified securely. Caution: bilateral procedure
Correct completion of all histological and radiological requests to pathology and radiology. This is especially important for intraoperative communication between the surgeon, pathologist, and radiologist.
Anesthesia: intubation or laryngeal mask
Positioning: upper body slightly elevated; pay special attention to the position of the arms (nerve injury).
Skin preparation, sterile draping of the operation region
Thoracic and axillary window; the contralateral breast should always be visible.
Operation
Simple Breast-Conserving Treatment
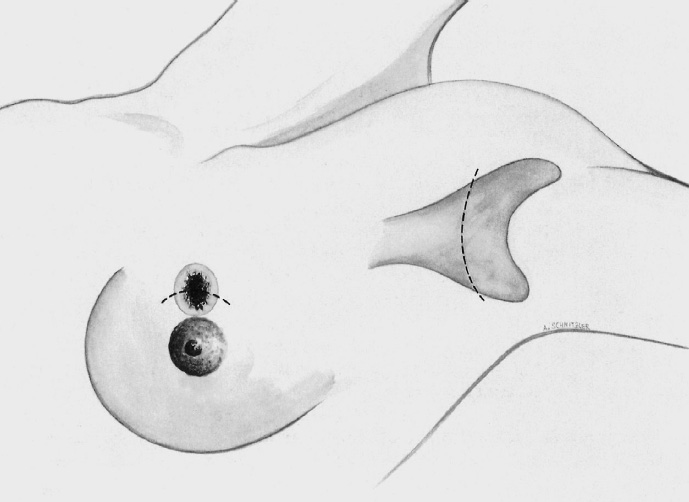
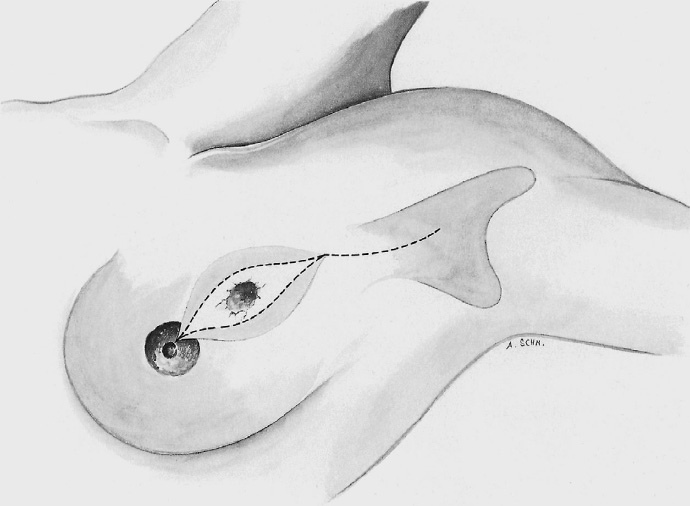
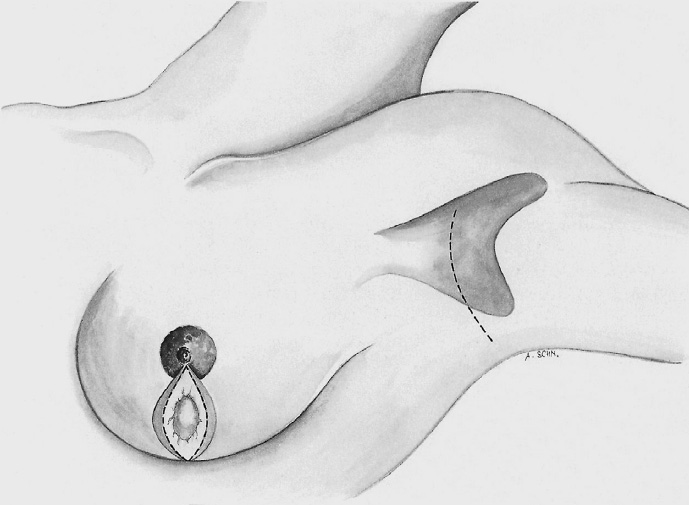
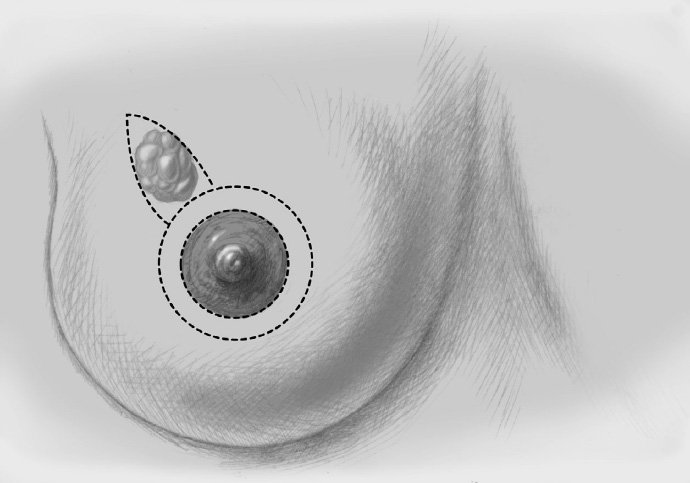
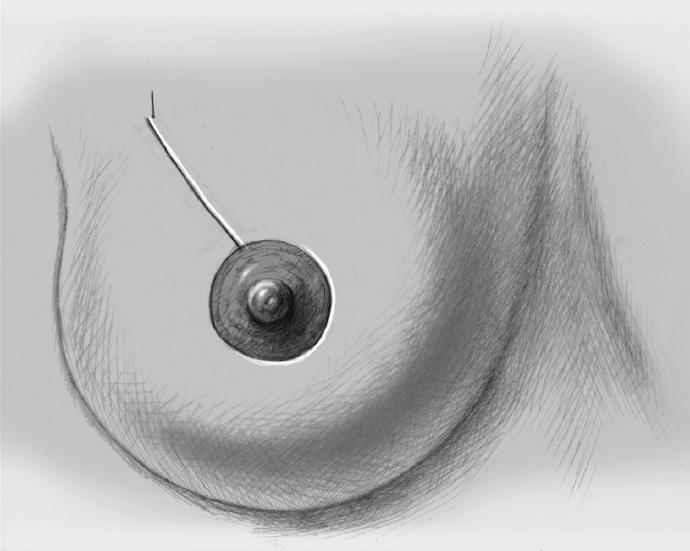
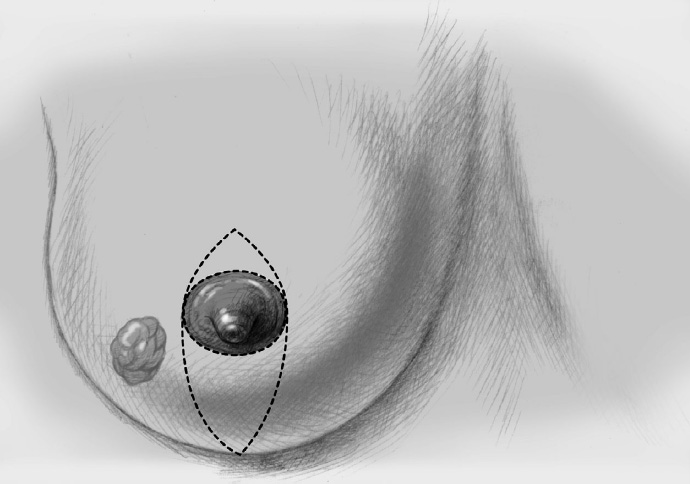
The skin is incised over the tumor region with or without skin excision (depending on surgeon, tumor size, tumor location, and subsequent treatment), often with a semicircular incision along the physiological (Langer) skin lines. A radial incision can be useful for tumors located in the lower quadrants or directly in the axillary tail of the breast. When there is a high risk of mastectomy initially, the incision should be within the ellipse of skin that will be removed at mastectomy. If the tumor is just beneath the skin, an island of skin over the tumor should be resected also. This can be achieved with both an elliptical semicircular incision and a radial incision.
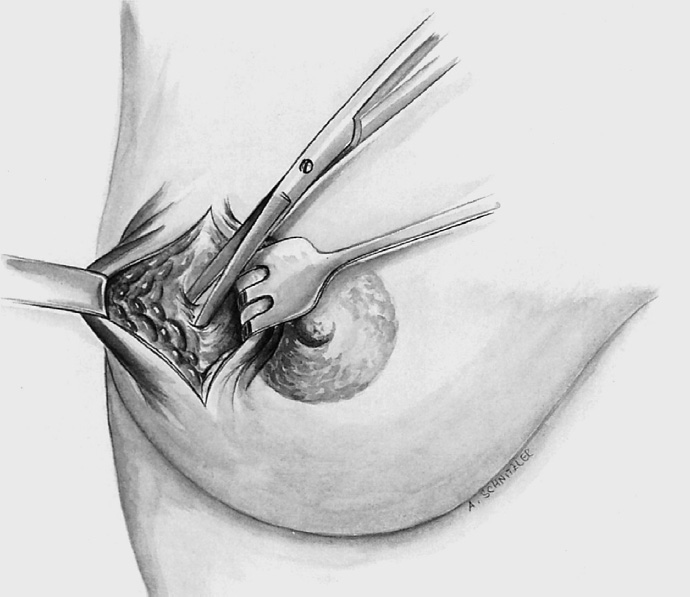
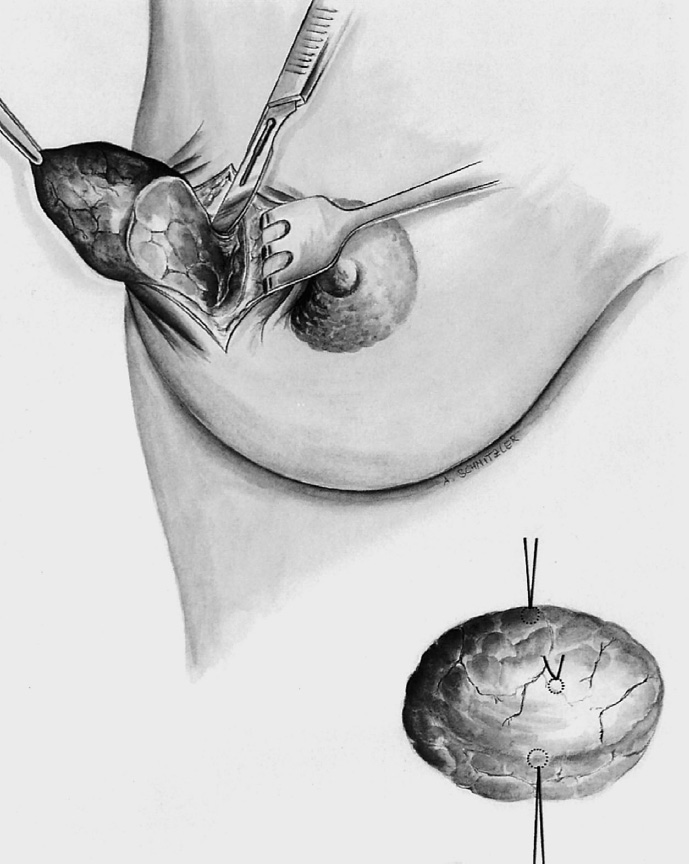
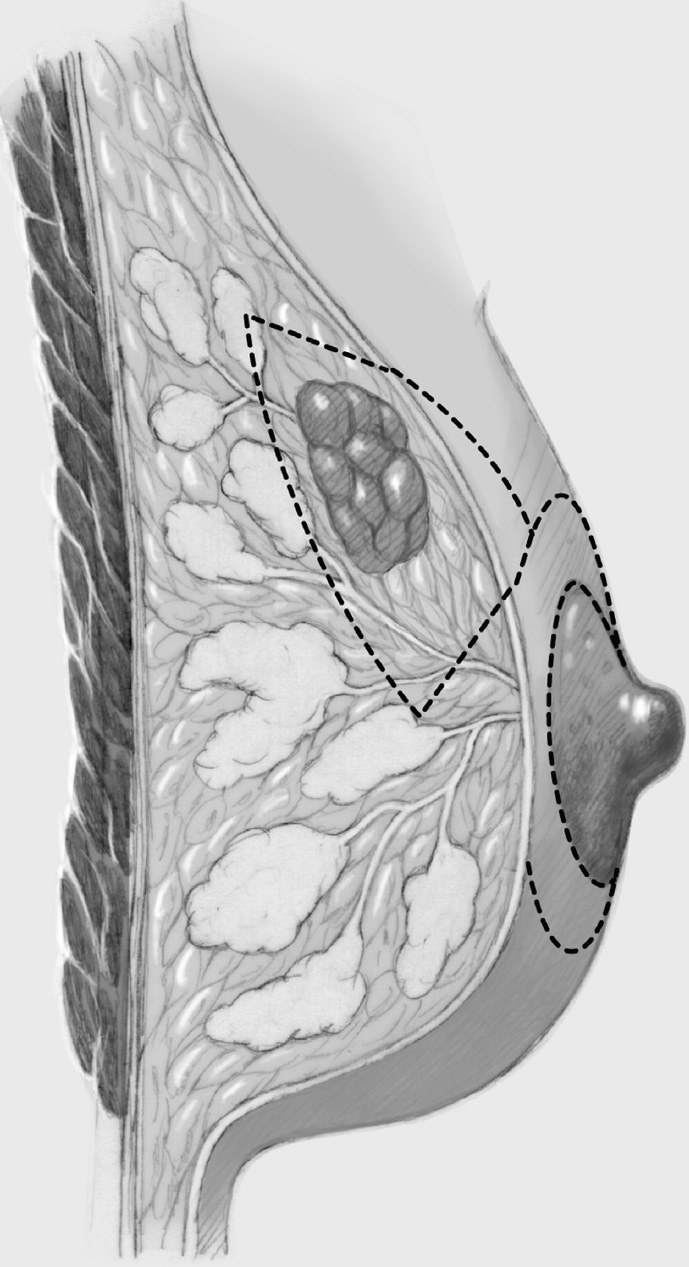
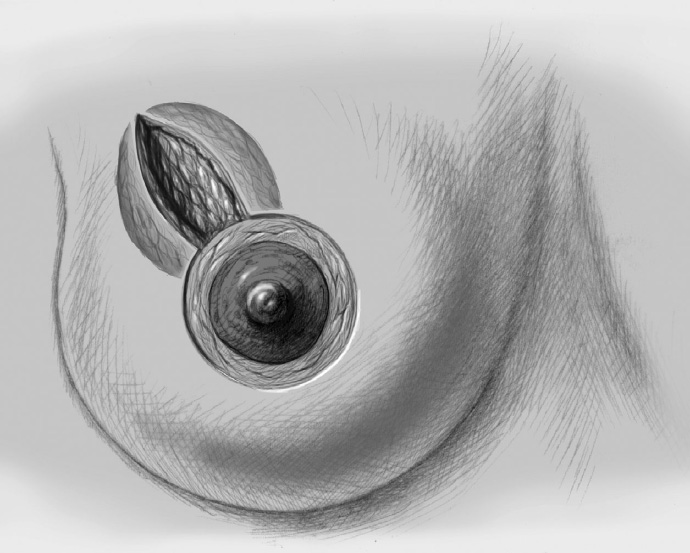
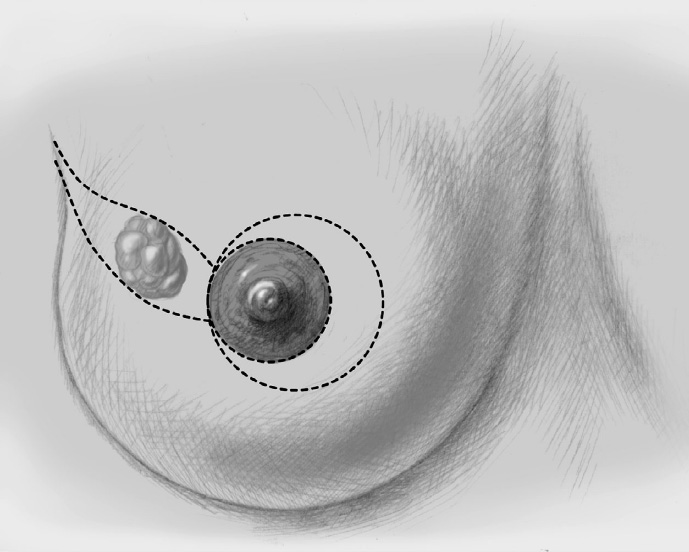
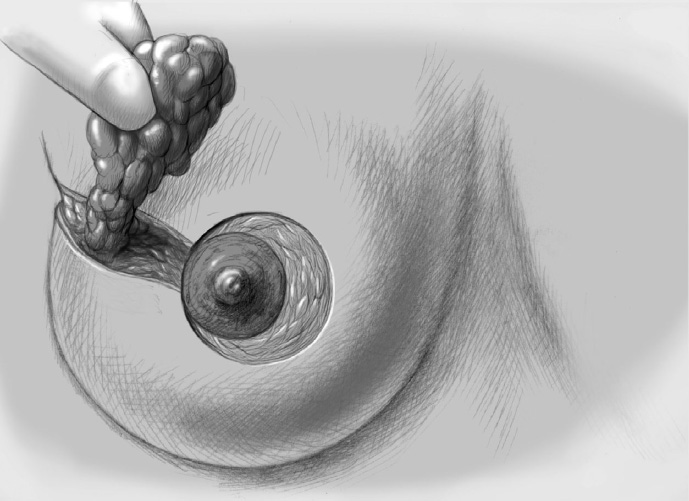
The segment containing the tumor is dissected sharply with dissecting scissors or electrocautery to obtain an initial adequate resection margin under digital control or sonographic direct visualization.
After complete resection of the segment containing the tumor, the specimen is marked with three sutures to provide precise three-dimensional spatial orientation for the pathologist, stating the exact location of the tumor in the breast (e.g., left breast at the 2-o’clock position, 5 cm from the nipple)—a specimen sonogram or mammogram is performed.
The tumor cavity is palpated digitally for further suspect areas. Further resection is performed if necessary, depending on the oncological situation (superior, inferior, medial, lateral, posterior, anterior). Digital palpation is naturally not an adequate pathological technique, not least because the induration of the tumor represents the stromal reaction around it and not the margins of growth of the soft tumor tissue. Nevertheless, a degree of experience is undoubtedly gained with palpation.
Hemostasis, insertion of a Redon drain
The tumor bed is marked with clips for accurate radiotherapy planning.
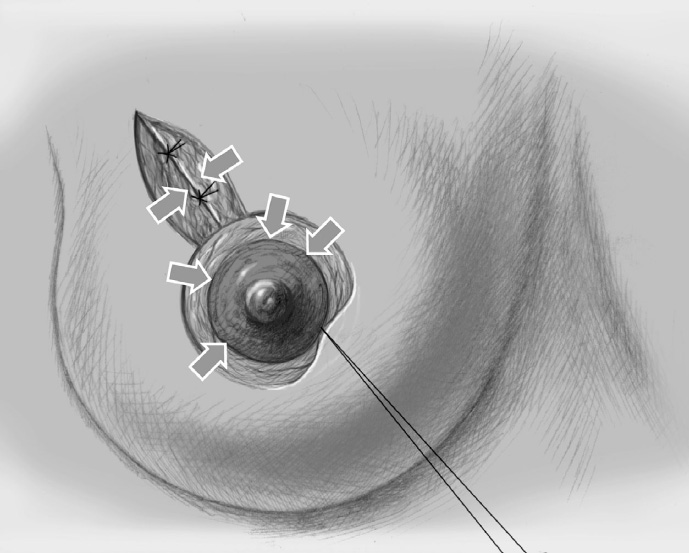
The breast tissue is approximated with Vicryl sutures (2–0). If the defect is small, little or no mobilization of the adjacent parenchyma is necessary (definition of “simple” BCS).
The wound is closed in two layers with a continuous intracutaneous suture.
Complex and Oncoplastic Breast-Conserving Treatment
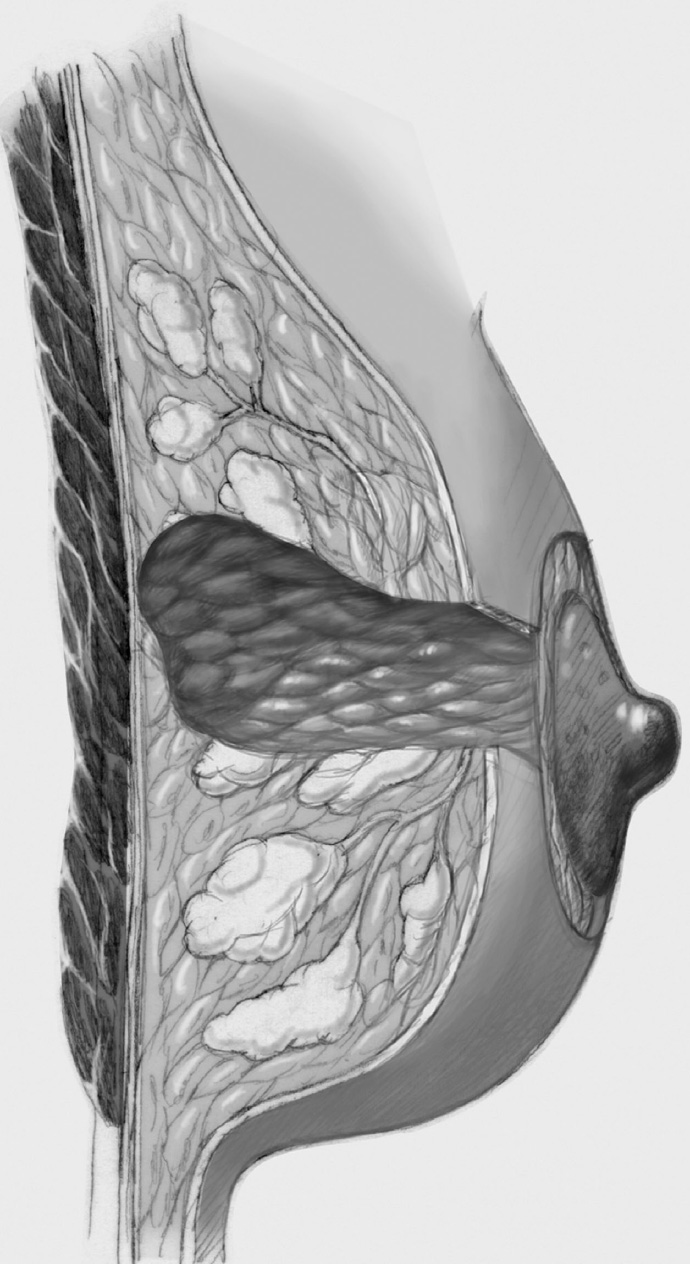
The same principles apply as in simple breast-conserving treatment though the size of the tumor necessitates more extensive segmental resection or even quadrant resection, which requires internal breast reconstruction with more complex defect cover by lobes of the breast. Often, more skin has to be resected to match the reduction in the size of the breast produced by the operation. Only the last step of periareolar de-epithelialization and nipple repositioning—that is, complex oncoplastic breast-conserving treatment—is not performed.
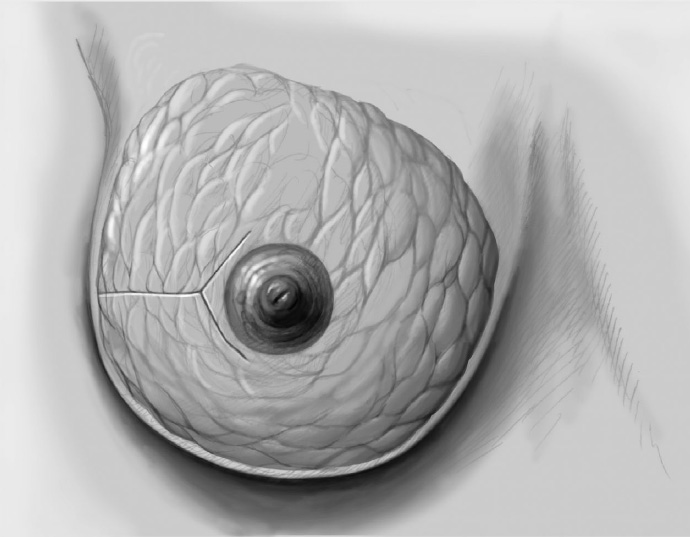
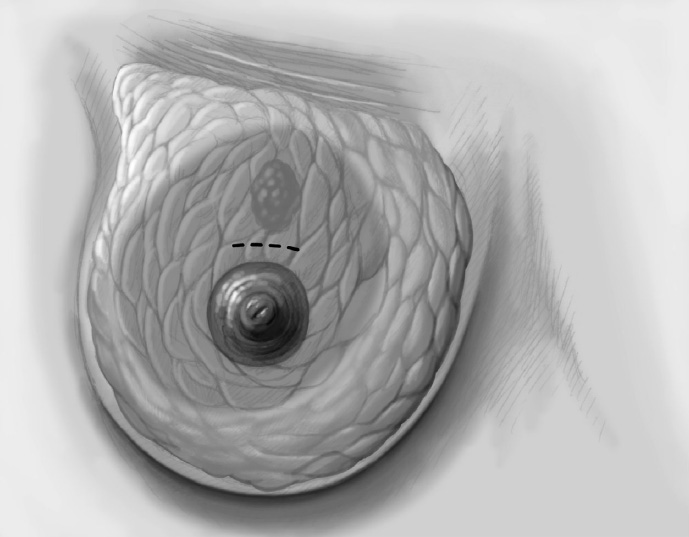
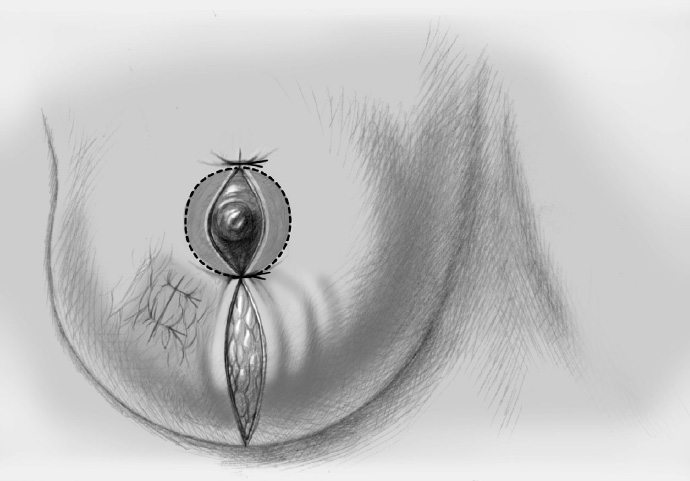
The skin is incised over the tumor region as far as possible (depending on surgeon, tumor size, tumor location, and subsequent treatment). A radial incision may be useful for tumors located in the lower quadrants or directly in the axillary tail of the breast. If the tumor is just beneath the skin, an island of skin over the tumor should be resected also. This can be achieved with both an elliptical semicircular incision and a radial incision. Another form is a purely periareolar incision when the tumor is in a relatively central position (see illustrations below).
The segment containing the tumor is dissected sharply with dissecting scissors or electrocautery; an adequate initial resection margin should be obtained under digital control or sonographic direct visualization. A specimen sonogram or mammogram is performed when needed.
After complete resection of the tumor area, a drain is placed in the wound cavity.
The former tumor region is marked with titanium clips (usually three clips for spatial orientation).
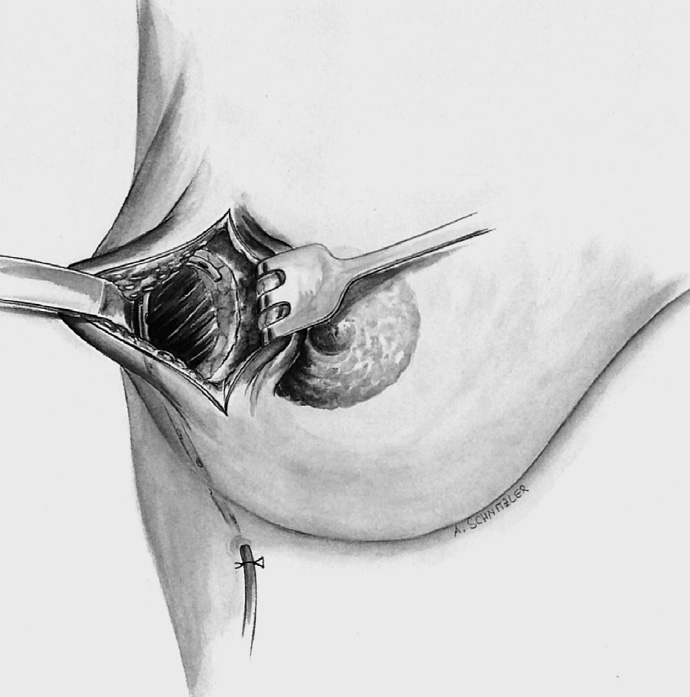
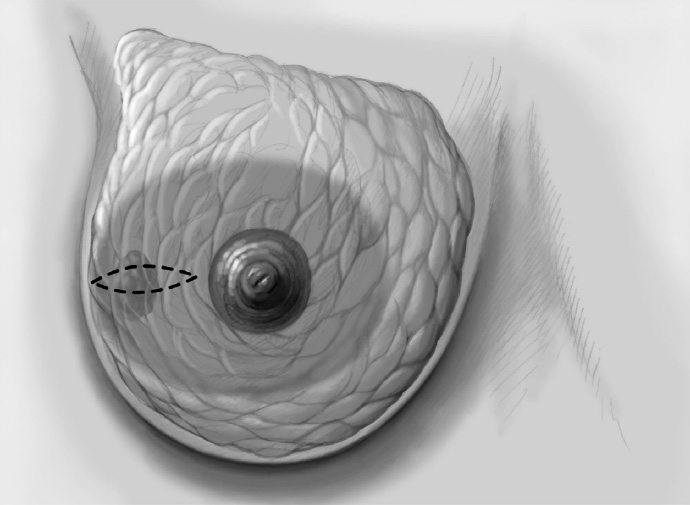
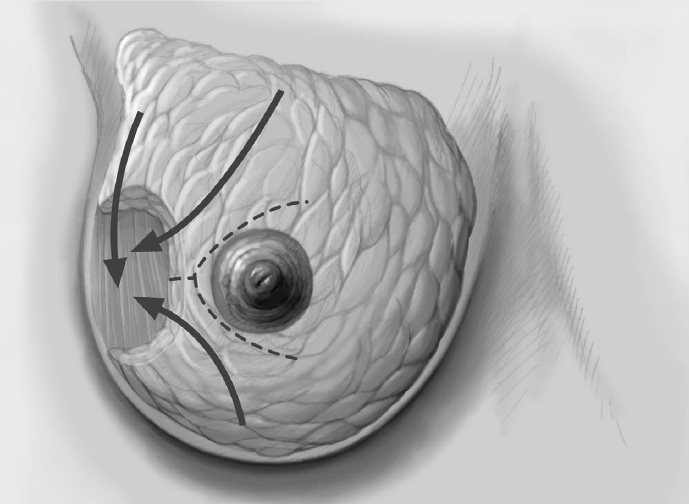
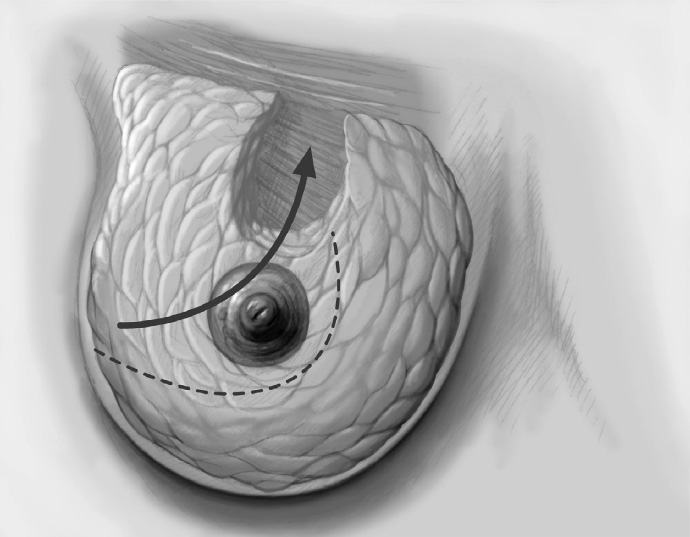
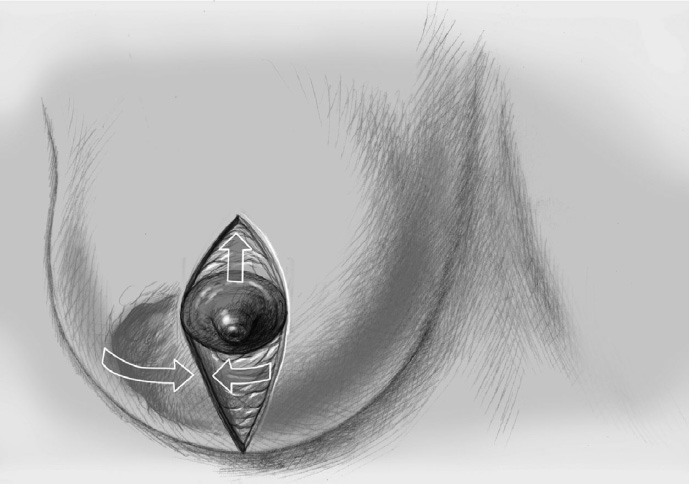
The adjacent parenchyma is mobilized subcutaneously so that the defect can be filled with lobes of breast tissue. Mobilization means exposing the breast relative to the skin or muscle to achieve adequate mobility of < 25% or > 25% as required.
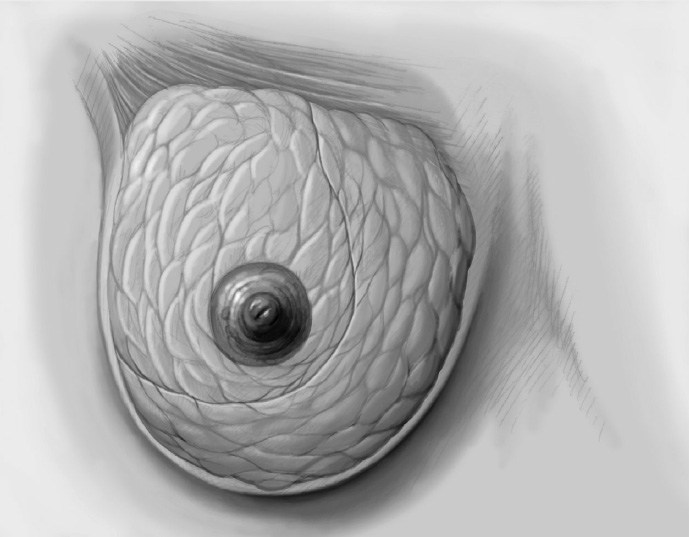
Tension-free approximation for complete intramammary cover of the defect
The wound is closed in two layers, suturing the skin with an absorbable monofilament (3–0 or 4–0) suture.
Special Technique Simple, Complex, and Oncoplastic Breast-Conserving Surgery
Complications
Secondary bleeding: Major intraoperative bleeding is rare. Secondary bleeding can always occur within the first 24 hours after surgery, though the overall incidence is low at < 2%. Secondary bleeding always requires revision and operative hemostasis.
Impaired wound healing: This is usually the result of local infection and occurs especially in the presence of risk factors such as smoking, diabetes, obesity, and immunosuppression.
Seroma: A postoperative seroma (< 5%) sometimes requires protracted management by frequent aspiration.
Scars: If the wrong operation technique is chosen when the tumor is large, the breast is small, and the breast–tumor relationship is unfavorable, ugly scarring and distortion may occur, with loss of an acceptable breast shape.
Scarring after radiotherapy: The new breast shape becomes “final” only several weeks after radiotherapy.
Concomitant and Postoperative Treatment
Local radiotherapy is mandatory after breast-conserving tumor resection; this is what constitutes breast-conserving therapy. The need for systemic postoperative treatment is guided by the final TNM status and depends on tumor size, nodal status, and histological parameters. The patient should mobilize promptly postoperatively with early drain removal (when secretion is < 30–40 mL/24 h) and appropriate physiotherapy following more extensive procedures. Every patient should be reviewed 10 to 14 days postoperatively and again before further treatment (radiotherapy and/or systemic therapy) is started.
Limits of the Methods
Preoperative planning with regard to necessary resection volume, tumor location, and the patient’s breast structure (shape, volume, parenchymal consistency, overlying skin) is crucial in complex BCS. With appropriate patient selection, simple BCS can produce excellent postoperative results. Conversely, inappropriate patient selection and poor preoperative planning can result in a very unsatisfactory postoperative situation, which is often difficult or impossible to correct.
3.2.2 Complex Oncoplastic Breast-Conserving Operations
Aims and Methods
Oncoplastic surgery. Oncoplastic surgery has become established in recent years, thereby increasing the rate of breast-conserving surgery and improving esthetic results. Oncoplastic means that surgery is not limited only to tumor excision but that the three important aspects of the breast are remodeled during the operation, namely, the breast gland itself, the skin, and the position of the nipple–areola complex. It combines resection in accordance with oncological principles and plastic surgical methods to cover or correct the defect. Deciding between breast conservation and mastectomy depends on classic factors such as the relationship between tumor and breast size and the condition of the breast (skin ptosis and breast density or atrophy), as well as on general contraindications. The surgeon’s familiarity with modern oncoplastic techniques is equally important. The fundamental and easily learned oncoplastic approaches (modified B-plasty, periareolar de-epithelialization, intramammary mobilization) should be part of every breast surgeon’s armamentarium. Although it would be desirable to provide guidelines for clinical situation → recommended operation, modern breast surgery is an extremely flexible field. Against the background of fixed rules regarding R status and established treatment guidelines, the surgeon’s skill and experience can provide a wealth of good surgical options; these are based on individual patient variables such as breast size and shape, degree of atrophy, patient age, size of the nipple–areola complex, degree of ptosis, micromastia, macromastia, existing asymmetry, individual wishes, tumor size, individual risks, and skin tension lines.
Operation classification. Although the principles of all breast-conserving surgical techniques are similar, it is important for scientific and didactic reasons, and not least for documentation, to use uniform nomenclature for these operations. The classification given in Chapter 1.2.2 distinguishes between “simple,”“complex,” and “oncoplastic” operations. The nomenclature then distinguishes further between complex oncoplastic breast-conserving surgery with periareolar de-epithelialization and movement of the nipple–areola complex, which is described below, and tumor-adapted mastopexy and tumor-adapted reduction mammoplasty (TARM, Chapter 3.2.3).
Indications and Contraindications
Indications
A primary complex oncoplastic procedure is indicated when the patient wishes for breast conservation and it is estimated that coverage of the defect without intraoperative nipple repositioning and skin adaptation would not lead in the long term to ugly distortion of the nipple–areola complex, and that the options for simple breast-conserving therapy are exhausted. This estimate is often based on the relationship between tumor size and breast size: tumor-adapted reduction mammoplasty is a possibility when the breast is large. “Typical” situations that require a complex oncoplastic procedure include large unifocal carcinomas, bifocal or multifocal carcinomas confined to one quadrant, and relatively large intraductal breast cancer that can still be treated with breast conservation. A small and drooping breast renders breast conservation difficult but a complex oncoplastic technique with skin tautening may be feasible.
Contraindications
The classic contraindications to breast conservation apply: multifocal and extensive carcinomas that do not allow adequate covering of the defect even when oncoplastic techniques are used. Inflammatory carcinoma and locally advanced tumors that require mastectomy are further contraindications. The possibility of postoperative radiotherapy is a precondition for breast conservation.
Operation Risks and Informed Consent
As in nearly all breast surgery, the general operation risks are wound infection, secondary bleeding, hematoma, seroma, scarring, nerve injury, and impaired sensation in the skin and nipple–areola complex. In particular, the patient must be informed of the postoperative change in the shape of the diseased breast and possible asymmetry compared with the healthy side. Plastic surgical correction of the healthy side must be planned, bearing in mind the pending postoperative treatment. Every patient must also be informed that further resection must be performed if resection margins are narrow or that mastectomy may be required if repeated secondary resection is necessary, extensive DCIS is present close to the tumor, and/or a multifocal carcinoma is found in the final specimen. The risk of local intramammary recurrence despite radiotherapy must also be discussed. Finally, the possibility of a poor cosmetic outcome and postoperative asymmetry must be addressed, especially in the case of marked breast ptosis or macromastia.
Operation Planning
All patients with histologically confirmed breast cancer should attend an interdisciplinary breast center to plan treatment and its timing.
Medical history, clinical examination (inspection and palpation), completion of histological diagnosis (if necessary), and diagnostic imaging
Imaging includes at least mammography and breast ultrasonography. MRI is indicated to exclude or confirm extensive or multifocal breast cancer, in the case of lobular carcinoma, and if dense breast tissue (grade 3 or 4) is found on mammography and/or ultrasonography.
Preoperative discussion of the patient by the breast team (breast surgeon, pathologist, and radiologist) and definitive planning of the extent of surgery. Determine the need for any neoadjuvant systemic therapy.
Discussion with the patient of the surgical procedure and potential risks
Patient’s consent to the procedure
The incision line is drawn with the patient standing or sitting up, either the day before or immediately prior to operation.
Thrombosis prophylaxis: low molecular weight heparin
Antibiotic prophylaxis: first or second generation cephalosporin
Moderately difficult to difficult operation because esthetically demanding; takes about 2 hours; surgeon and one assistant
Anesthesia and Positioning
Special Instruments
Breast set: dissecting scissors, electrocautery knife, electrocautery needle, skin hooks, Roux hooks
Procedure
Preparation
The patient should empty her bladder immediately before transport to the operating room.
The patient and the breast to be operated are identified securely. Caution: bilateral procedure
Correct completion of all histology requests to pathology
Anesthesia: intubation or laryngeal mask
Positioning: slight elevation of the upper body; pay special attention to the position of the arms (nerve injury); allow for the possibility of bringing the patient into a semi-sitting position during the operation.
Skin preparation, sterile draping of the operation region
Thoracic and axillary window; the contralateral breast should be visible for overall assessment.
Operation
Complex Oncoplastic Breast-Conserving Treatment
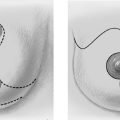
The basic decision on whether to use a complex oncoplastic technique is made when the skin is marked preoperatively, with the patient standing or sitting upright. Many surgeons successfully combine the B-plasty incision with periareolar de-epithelialization and excision of a straight or curved ellipse of peripheral skin (Chapter 1.3). When marking the periareolar deepithelialization pattern, an eccentric incision may be necessary to adjust the repositioning of the nipple–areola complex to the anticipated volume displacement.
The skin is incised superficially along the preoperative mark, initially with a scalpel. Many surgeons then proceed using electrocautery needle or scissors.
The periareolar skin is de-epithelialized. Here, too, there are various options. A strip of the most superficial skin layer can be excised with dissecting scissors applied flat or with a scalpel. It is important not to leave behind any surface containing squamous epithelium, but on the other hand the dermis and the important vascular layer beneath it must not be injured. The purpose of periareolar de-epithelialization is to recenter the nipple–areola complex and also to tailor excess skin to the new breast shape following extensive tumor resection.
Segmental excision of the area containing the tumor with resection margins as wide as possible to meet oncological criteria. Oncoplastic techniques should be used to achieve maximal oncological safety and avoid subsequent further resection.
Further resection is performed if necessary to ensure R0 status.
The former tumor region is marked with clips.
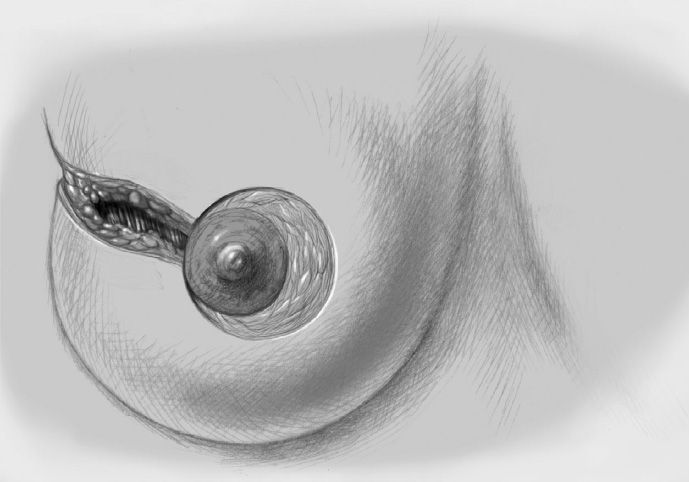
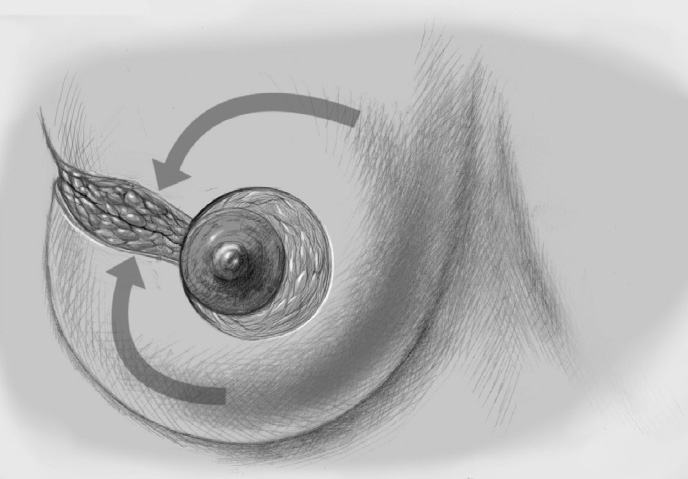
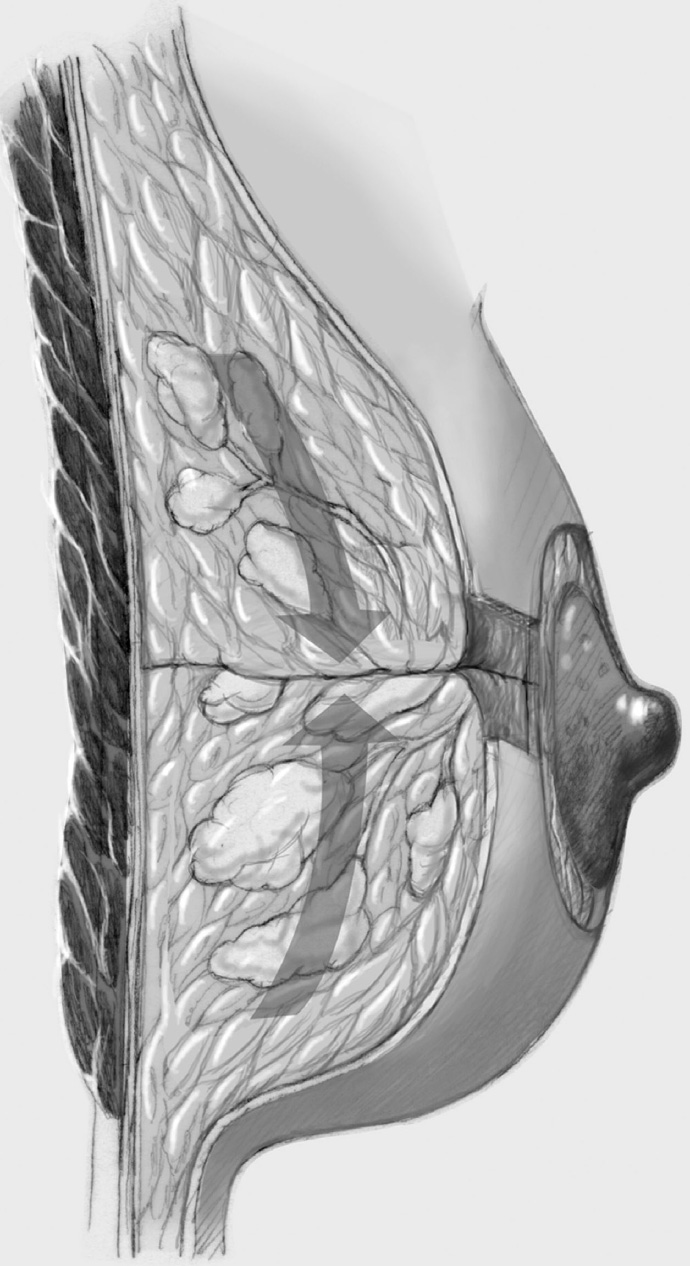
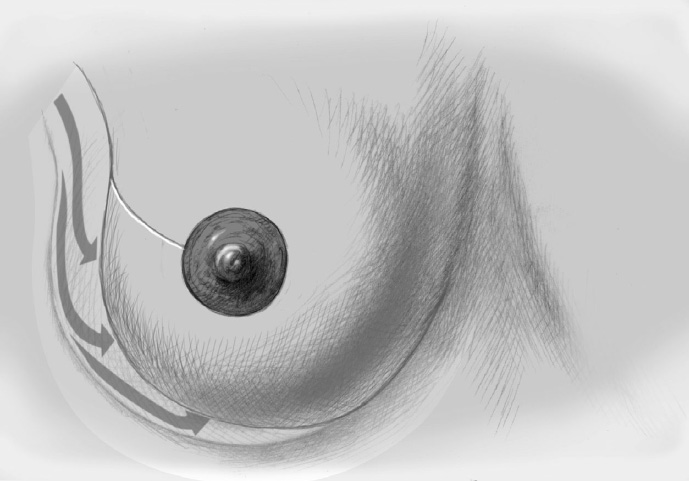
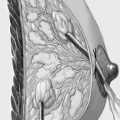
To cover the defect, the glandular lobes are mobilized from the adjacent parenchyma after subcutaneous dissection. The principle of intramammary lobe creation is to mobilize large parts of the breast (> 25%) either relative to the skin or relative to the pectoralis muscle. This “liberation” of the breast from one of its two planes of fixation allows adequate dissection and rotation of sufficient breast tissue. The Y-flap and rotation flap shown in Chapter 3.2.1 are examples of intramammary dissection.
When the breast is mobilized subcutaneously, it must be ensured that both the dissected skin layer and the breast tissue are sufficiently thick. For the layer of breast tissue, a minimum thickness of 1 cm is desirable. The ratio of base to length must also be considered.
The former tumor bed is marked with clips for optimized postoperative radiotherapy.
A Redon drain is placed prior to approximation of the breast lobes.
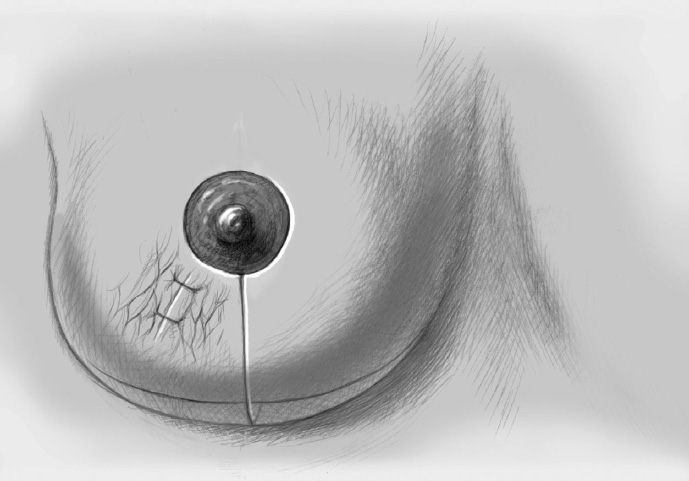
The mobilized breast lobes are rotated into the defect and approximated by interrupted sutures. Complete covering of the defect is desirable.
The skin is closed in two layers with recentering of the nipple–areola complex using interrupted sutures (Vicryl 3–0) according to the preoperative de-epithelialization pattern, which can be corrected at this time.
The skin is closed with an intracutaneous continuous monofilament suture.
Special Technique Complex Oncoplastic Breast-Conserving Surgery
Complications
Bleeding: Major intraoperative bleeding is rare. Secondary bleeding can occur within the first 24 hours after surgery, though the overall incidence is low at < 2%. Secondary bleeding always requires revision and operative hemostasis. Skin bruising may occur but disappears with time (2–3 weeks) and is of no surgical consequence.
Impaired wound healing: This is usually the result of local infection, especially in the presence of risk factors such as smoking, diabetes, obesity, and immunosuppression.
Seroma: A postoperative seroma may be a complication and sometimes requires protracted management by frequent aspiration.
Scars: If the wrong operation technique is chosen when the tumor is large, the breast is small, and the breast–tumor relationship is unfavorable, ugly scarring and distortion may occur, with loss of an acceptable breast shape. Keloid scars may also occur.
Scarring after radiotherapy: The new breast shape becomes “final” only a few weeks after radiotherapy.
Liponecrosis: Liponecrosis may occur, especially after extensive parenchymal mobilization and when the breast has undergone fatty involution.
Concomitant and Postoperative Treatment
Local radiotherapy is mandatory after breast-conserving tumor resection; this is what constitutes breast-conserving therapy. The need for systemic postoperative treatment is guided by the final TNM status and depends on tumor size, nodal status, and histological parameters. The patient should mobilize promptly postoperatively with early drain removal (when secretion is < 30–40 mL/24 h) and also appropriate physiotherapy following more extensive procedures. Every patient should be seen again 10 to 14 days postoperatively and before the start of further treatment (radiotherapy and/or chemotherapy). If there has been a substantial reduction in ipsilateral breast volume, the healthy breast can be altered either during the primary surgery or following conclusion of the radiotherapy and/or chemotherapy, according to the patient’s wishes.
Limits of the Methods
Preoperative planning with regard to the resection volume, tumor location, and the patient’s breast structure (shape, volume, parenchymal consistency, overlying skin) must be as accurate as possible, as this is crucial in complex breast-conserving surgery. If the resection volume exceeds one quadrant, breast-conserving surgery is often no longer possible with oncological safety. Incorrect assessment of the patient and poor preoperative planning can likewise lead to unsatisfactory postoperative situations that are often difficult to correct. Despite the enthusiasm for these techniques and the greatly expanded options for breast-conserving surgery, the limit of what is oncologically acceptable should therefore not be exceeded. Mastectomy continues to be indicated in this case.
The oncologically necessary resection volume must always be considered in relation to the volume and structure of the breast. Guaranteeing oncological safety with regard to recurrence is the most important aspect of breast-conserving therapy. As mentioned above, the resection margins should be > 1 mm with invasive carcinoma and > 2 mm with DCIS.
3.2.3 Complex Oncoplastic Breast-Conserving Surgery with Additional Reduction Mammoplasty (TARM)
Aims and Methods
The principles of breast-conserving surgery combine an optimal esthetic result with maximum oncological safety. The relationship between tumor size and breast size is an important factor in deciding on the best operation technique, but the shape of the breast and the initial esthetic situation must also be considered. Particularly large breasts are suitable for a breast-conserving procedure as adequate breast parenchyma can be mobilized to fill even large intramammary defects. However, two problems have emerged in the last 20 years: on the one hand, it became clear that while large breasts appeared at first glance to meet the requirements for conventional simple breast-conserving surgery, they did not do so in the long term. Second, radiotherapy of large breasts is not easy (with radiation fibrosis) and radiotherapy has a high complication rate together with reduced oncological safety. As an excessively large breast is troublesome for the patient, both cosmetically and functionally, reduction of breast volume as part of breast cancer therapy has generally become accepted. This is referred to as tumor-adapted reduction mammoplasty (TARM). Over the last 20 years, numerous modifications of breast reduction based on the classic McKissock plastic surgical technique (vertical pedicle) have become established, offering the surgeon a wide choice of options. It is obvious that the parts of the breast to be resected should include the cancer, removing this with adequate oncological safety margins. This option has become an integral part of complex oncoplastic breast surgery in the last 10 years and, together with contralateral reduction immediately or following radiotherapy, is now a new treatment approach for many breast cancer patients.
Indications and Contraindications
The indications and contraindications correspond to those of other breast-conserving procedures. A precondition is histological confirmation of an invasive tumor or premalignant lesion warranting surgery, and clinical and imaging evidence that the process is unifocal or limited to one quadrant. The patient’s desire for breast conservation, accepting the necessity of postoperative radiotherapy, is crucial. The usual contraindications (e.g., inflammatory carcinoma, no possibility of postoperative radiotherapy) apply. Absolute or relative macromastia and the patient’s consent to breast reduction are obvious requirements.
Operation Risks and Informed Consent
The patient must be informed of the usual risks such as bleeding, hematoma, wound infection, suture dehiscence, and scarring. These risks are somewhat increased, at least theoretically, because of the physiological circumstances (macromastia), but also as a result of the more complex and extensive dissection for TARM. Wound healing is impaired in smokers, diabetics, and in patients on long-term corticosteroid therapy. The rationale for breast reduction with regard to the complications of postoperative radiotherapy of a large breast should be explained. The incision and postoperative appearance, including the possibility of an ugly scar, should be demonstrated and discussed. As with all breast-conserving procedures, these operation risks should be balanced against the advantages and disadvantages of the surgical alternative of mastectomy with or without heterologous or autologous reconstruction. The long-term possibility and/or (esthetic) advisability of contralateral breast reduction with its attendant surgical risks should also be addressed.
Operation Planning
Breast cancer surgery and treatment planning is largely standardized:
Medical history, clinical examination (inspection, palpation)
Imaging: breast ultrasonography and mammography; breast MRI in selected cases (e.g., to exclude or confirm a multifocal lesion, ACR 4 breast [Chapter 1.4.4], lobular carcinoma on histology)
Histological confirmation by minimally invasive breast biopsy (mammographic, ultrasound-, or (rarely) MRI-guided)
Detailed discussion and treatment planning with the patient following confirmation of the histological diagnosis
Preoperative staging to exclude distant metastasis is required today only if this is suspected clinically or the tumor is at an advanced stage.
Decisions on treatment are made along the critical axis of neoadjuvant versus adjuvant therapy, breast conservation versus mastectomy, mastectomy with or without reconstruction, heterologous versus autologous reconstruction, and need for radiotherapy.
Because of the plastic surgical approach, elements of the preparation for conventional (noncancer) reduction mammoplasty are adopted: detailed demonstration of the situation with explanations for the patient (degree of ptosis, asymmetry, chest wall anatomy and its significance for the breast outline, differences in size). This should include photodocumentation.
Discussion of different surgical techniques with illustration (using photos) of possible results, both ideal and also average and less successful results
Like cosmetic breast reduction, tumor-adapted reduction mammoplasty requires careful measurement of the breast and consideration of certain parameters for reconstruction: the nipple–areola complex should be about 20 to 23 cm from the sternal notch, be roughly in the midclavicular line, and be approximately 4 cm in size. The lines joining the nipple–areola complexes on either side and the sternal notch should produce an approximately equilateral triangle. The lower border of the areola should be at the level of the submammary fold, that is, 5 to 6 cm from the chest wall. These measurements should result in the nipple–areola complex being at about the level of the center of the upper arm or slightly lower.
The treatment plan is established and the patient is provided with information about the chosen operation.
Consent to the procedure
The incision is marked preoperatively with the patient standing, the day before the operation or immediately prior to operation, checking that the correct side is marked.
Anesthesiological preoperative investigations depending on the patient’s age and local practice
Thrombosis prophylaxis: low molecular weight heparin
Antibiotic prophylaxis: first or second generation cephalosporin
Difficult surgery; takes 3 to 4 hours; surgeon and one assistant
Anesthesia and Positioning
Special Instruments
Breast set: dissecting scissors, electrocautery knife, electrocautery needle, suction, skin hooks, Roux hooks
Forceps, clamps (Käser–Duvall), Russian forceps, especially when concomitant axillary lymph node dissection is performed
Procedure
Preparation
The incision is marked on the day before the operation or immediately prior to the operation with the patient standing.
If a bladder catheter is not placed, the patient should go to the toilet before transport to the operating room.
The patient is identified in the pre-op and operating room: check that file and patient match; patient confirms the planned operation according to the entry in her file and the preoperative marking.
Intubation versus laryngeal mask
Positioning: semi-sitting positions are favored by many surgeons, arms abducted bilaterally
Skin preparation, sterile draping: thoracic access
Operation
The various intramammary pedicles and different incisions for appropriate reduction of the overlying skin are shown in the chapter on reduction mammoplasty (Chapter 3.3.2). The classic modern pedicles (inferior central, superior, and purely central) with the corresponding incisions (inverted T, short inferior incision [vertical periareolar], and periareolar) are presented below.
Inferior Central (Central Caudal) Pedicle with Inverted T Incision
Among reduction mammoplasties, this technique is regarded as relatively low-risk and is therefore suitable also in smokers and older postmenopausal patients (impaired perfusion). Because the breast volume may be reduced by more than 50%, the method can also be used when the breasts are very large. The approach is suitable especially for tumors in the upper quadrants, central tumors, and tumors in the upper part of the lower quadrants.
The incision is usually the classic McKissock one, finally resulting in an inverted T scar, though the inferior pedicle (which will be de-epithelialized) is kept somewhat broader (as a guide, the scalpel shaft length is approximately 8–10 cm), because this bears and supplies the nipple–areola complex without an additional superior pedicle.
The new anterior nipple position is established, initially only by “impingement” of a finger in the submammary fold, but without excising the nipple. Caution: Because of the frequent postoperative retraction of the reduced skin, the new nipple position may be too high if the surgeon keeps too strictly to the distances recommended in the literature and is guided too little by the individual situation.
To avoid excessive tension of the skin envelope, especially in the submammary fold, it is advisable to raise limbs longer than 7 cm (around 9–10 cm) and resect the resulting excess skin later, prior to skin approximation. The nipple position should also be established only after submammary suture to avoid an excessively cranial position.
The long-term target distance between nipple and submammary fold is approximately 7 to 8 cm, and the distance between the sternal notch and nipple should be 19 to 23 cm. The described procedure should achieve these classic distances after wound healing and skin retraction.
Following the skin incision, the superior skin envelope is dissected off the breast, that is, in a superior, medial, and lateral direction. This step is crucial as it provides maximum access to the breast, enabling reduction to be “tailored” exactly to the tumor.
The breast containing the tumor is resected in classic segmental fashion along the tumor axis. In purely cosmetic reduction, tissue is removed mainly in the upper outer part and somewhat less in the superior and medial part. It is important to leave sufficient breast tissue behind the areola and in the cranial part as otherwise the projection of the areolar region will be poor after it is sutured. Additional tissue can be resected lateral to the inferior pedicle on right and left.
The skin is approximated subdermally in the region of the vertical limb in preparation for reconstruction of the reduced breast with chest wall fixation and repositioning of the nipple.
The breast is fixed to the pectoralis muscle to avoid postoperative lateral deviation of the “new” breast. The de-epithelialized dermis covering the inferior central pedicle is sutured to muscle in a superolateral and superomedial direction using absorbable sutures (Vicryl 0, 2–0). It is useful to draw down the new skin envelope over the “new” breast to determine its optimal position on the chest wall.
The skin envelope is again peeled off the breast and excess skin is excised, in an inferomedial and especially inferolateral direction.
After establishing the final position of the nipple–areola complex, the marked area of skin is excised precisely over the nipple. To facilitate positioning, a retaining suture can be placed in the nipple at the 12-o’clock position; this allows assessment of any tension on the nipple (e.g., due to the internal fixation). Following skin excision, the nipple can be readily guided to its new position using the retaining suture.
A drain is inserted and the skin is closed in two layers.
Surgeons differ greatly in their postoperative dressing preferences.
Superior Pedicle
This technique can be employed when the tumor is in an inferior and central location (lower quadrants), ideally when the macromastia is moderate.
Marking the incision line is particularly difficult as gathering the skin along the vertical axis (midclavicular line) determines the ultimate breast contour. The new nipple–areola complex cannot be planned as exactly preoperatively as with an inferior central pedicle. The incision is usually periareolar and vertical (or perivertical). The subsequent operation, with slight variants, is also known as the LeJour technique and becomes the Marchac technique if it is extended to a small inverted T.
Inferior and central posterior breast tissue is mainly resected. As in all tumor-adapted procedures, dissection continues down to the pectoralis major muscle, elevating the residual breast in the superior direction. The final step is “retrograde” resection in the upper part of the breast also, which is important for the final shape of the breast. Nevertheless, the technique is not the first choice when the tumor is located in the upper quadrants.
The nipple is repositioned at the most cranial point of the measured periareolar de-epithelialization area. If nipple repositioning over a long distance is necessary, a domelike extension in a cranial direction can be de-epithelialized beyond the purely periareolar de-epithelialization area (LeJour technique).
Central Pedicle—Purely Periareolar Approach
Tumor-adapted reduction mammoplasty can also be performed with a central pedicle. In this case, the intramammary procedure is usually combined with a periareolar incision to reduce the skin envelope. Segmental extension of the incision is possible, not unlike the modified B-plasty incision. The requirements are good vascularization and elastic skin that is capable of shrinking (because of the problem of “excess” skin in the suture area). Up to 50% of the breast volume can be resected. The technique is more suitable for use in young women. This approach can be used for generous segmental resection of tumors that are not too peripheral or too close to the skin.
The first step after marking the incision line is periareolar de-epithelialization.
The breast is exposed completely, starting from the wide de-epithelialized ring, by dissecting the skin off it in circular fashion. The skin is elevated from the breast superiorly and inferiorly, leaving a roughly 1-cm layer of subcutaneous fat.
Some authors advise against dissecting this layer down to the pectoralis fascia in order to protect the nerves and vessels coursing on the chest wall. However, exposure of the pectoralis muscle is useful for modeling the breast. The perforating vessels at the periphery running from the muscle into the subdermal plexus must on no account be injured.
The tumor is resected oncologically from the exposed breast with further resection if necessary. Circular reduction of the breast is performed in addition, ensuring that the central pedicle is not narrowed to an hourglass shape.
For internal modeling, it is advisable to reshape the reduced breast with interrupted sutures and fix it to the chest wall, especially medially, laterally, and superiorly.
As in all reduction mammoplasties, insertion of suction drains is recommended. The inferior part of the wound in particular must be drained for long enough as removing the drain too soon can lead to seroma development and delayed wound healing.
The bigger, outer ring of skin is approximated to the smaller inner ring: a gathering subdermal purse string suture is placed along the outer ring, largely adjusting this to the smaller inner ring. This is followed by the normal two-layer approximation. The excess skin shrinks well when it is sufficiently elastic.
The technique can be modified with a periareolar incision with segmental (medial or lateral) or vertical (inferior) extension. If the diameter of the periareolar ring becomes greater than 10 cm, this extension is advisable, as the extreme creasing of the skin produced when the ring is bigger persists even after healing. Segmental or vertical extension and skin resection makes the ring smaller and leads to further tautening of the skin.
Segmental extension in particular enables skin directly over the tumor to be resected with more direct and visible removal of the invasive lesion.
Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


