Introduction
The soft tissue layers of the face from the surface down are generally made up of the skin, subcutaneous fat, superficial fascia (superficial musculoaponeurotic system [SMAS]), mimetic muscles, and deep tissue layers. Structurally, these layers vary among the different regions of the face. For example, the subcutaneous fat layer does not exist in the eyelid, lip, or nose. The deep tissue layer is covered by deep fascia and includes the parotid gland, masseter muscle, buccal fat pad, deep temporal fascia, and temporalis muscle. The structures within the deep tissue layer also vary among the different facial regions. Each layer is connected to adjacent layers and supports proper anatomical positioning of the facial soft tissue against gravity. Among the soft tissue layers of the face, the SMAS is the key structure of the facial fascial system. This chapter describes the basic structure of each layer and presents cadaver dissections and microscopic images.
Subcutaneous Fat Layer
The subcutaneous fat is located beneath the dermis and is present throughout most of the entire body. In body regions other than the face, the subcutaneous fat layer is divided into two layers by the superficial fascia, and each layer exhibits different characteristics. The superficial fat layer contains many fibrous septa and is involved in protection from external forces. Nakajima et al1 termed this fat layer the protective adipofascial system. In contrast, the deep fat layer provides flexibility to musculo-skeletal movement and is termed the lubricant adipofascial system. The facial subcutaneous fat contains many fibrous septa and has a structure similar to that of the protective adipofascial system. The subcutaneous fat layer has an intimate relationship with the SMAS. Many connective tissue fibers rise upward to the dermis and provide a strong connection between the dermis and SMAS. Each lobule of the subcutaneous fat is small and surrounded by dense fibrous septa. In the cheek region, a thick fat tissue layer lies on the SMAS and is distinct from the subcutaneous fat layer. This fat tissue is called the malar fat pad.
Malar Fat Pad
The malar fat pad is the fat tissue that lies superficial to the SMAS in the cheek region. It is triangular shaped and bound medially along the nasolabial crease, superiorly along the orbital rim, and laterally along the convex curved line connecting the lateral canthus and nasolabial crease around the corner of the mouth. At the location of the malar fat pad, the upper half of the SMAS comprises the orbicularis oculi muscle, and the lower half comprises the superficial upper lip elevator muscles. The lower half of the SMAS is quite thin and almost discontinuous and has no mechanical bearing capacity. The malar fat pad is firmly fixed to the dermis and relatively loosely fixed to the SMAS layer in this region. The zygomatic ligament, which is an osteocutaneous ligament located on the zygoma lateral to the origin of the zygomatic minor muscle, inserts in the overlying dermis and pierces and anchors the malar fat pad to connect it to the deeper tissue layers.
Cosmetically, the malar fat pad slides downward and inward over the SMAS with aging, deepening the nasolabial crease. Fat tissue is also present beneath the orbicularis oculi muscle. This fat tissue is called the suborbicularis oculi fat pad and lacks continuity with the malar fat pad.
SMAS
The SMAS is the fascial tissue layer located just beneath the subcutaneous fat layer. It connects the facial muscles with the dermis, transmits contraction of the facial muscles to the skin, and assists in creating facial expression. The SMAS is the key structure in surgical treatment of the face, and an accurate knowledge of its anatomy is extremely important. The existence of superficial fascia in the head and neck region has been discovered in fragments; for example, the superficial temporal fascia and galea aponeurotica were not originally recognized as a continuous layer. The concept of a fascia layer that spreads throughout the entire head and neck region in one sheet and is integrated with the conventional fragmental fascial structures (i.e., the concept of the SMAS) was first advocated by Mitz and Peyronie in 1976.2 The SMAS is a fascial layer that is connected superiorly to the frontalis muscle and inferiorly to the platysma muscle. Its thickness decreases as it continues to the anterior cheek area. Although some opinions differ, the generally prevailing thoughts regarding the SMAS are almost identical to those proposed by Mitz and Peyronie.2
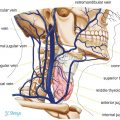
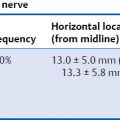
The SMAS lies on the same horizontal plane as the platysma muscle and extends superiorly to the superficial temporal fascia, galea aponeurotica, and frontalis muscle in its upper region (Fig. 11.1). However, some authorities have questioned the continuity of the SMAS in the temporal region. Gosain et al3 reported that the SMAS terminates within 1 cm below the zygomatic arch and is not continuous with the temporoparietal fascia (superficial temporal fascia). Intraoperatively, the area over the zygomatic arch has a complicated structure. The superficial temporal artery passing from the deep plane to the superficial temporal fascia layer and the temporal branch of the facial nerve also passes from the deep layer to the inferior surface of the superficial temporal fascia. The SMAS is also difficult to dissect as a uniform layer. It is quite thick in the parotid–masseteric and zygomatic areas and is easily dissected in this region under gross visualization. Beyond the anterior border of the masseter muscle, however, the SMAS becomes quite thin and almost invisible, making it quite difficult to dissect, raising questions about the continuity of the SMAS. Gardetto et al4 stated that the SMAS cannot be detected in any facial region other than the parotid region. Jost and Levet5 questioned whether the SMAS actually continues to the orbicularis oculi muscle from an embryologic point of view. The orbicularis oculi originates from the sphincter colli profundus; however, the platysma muscle, which lies on the same plane as does the SMAS, originates from a different layer (i.e., the platysma layer). Thus, confusion results from the histologic differences among the soft tissue layers of the lateral and central facial regions. Ghassemi et al6 claimed that the SMAS can be histologically classified as type 1 or type 2. Type 1 SMAS describes the common architecture of the posterior part of the face and is observed in the forehead, parotid region, zygomatic region, infraorbital region, and lateral aspect of the nasolabial fold. The subdermal structure comprises a mesh-work of fibrous septa enveloping lobules of fat cells. Type 2 SMAS is found in the upper and lower lips, and the subdermal tissue comprises a meshwork of intermingled collagen, elastic fibers, and muscle fibers.
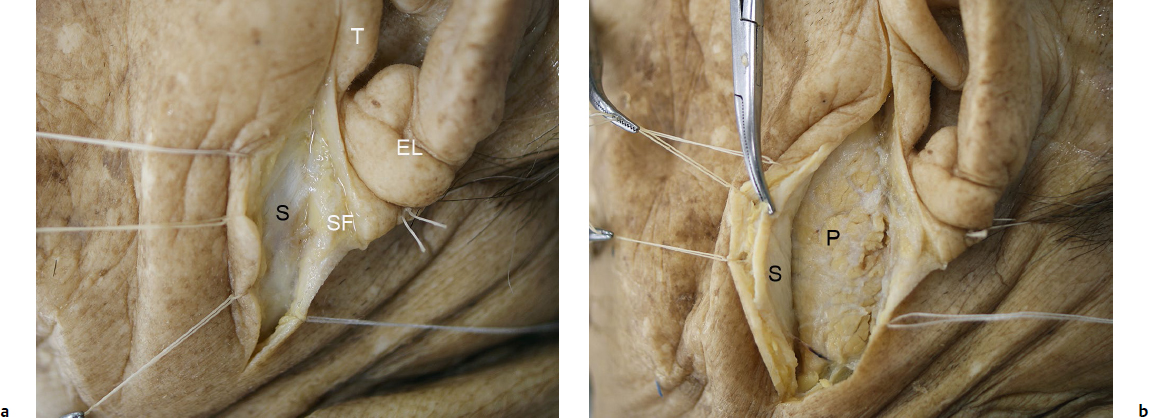
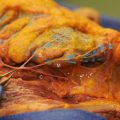
Fig. 11.1 Cadaveric dissection of the superficial musculoaponeurotic system (SMAS) in the parotid region. (a) The SMAS is seen as a white fibrous layer under the subcutaneous fat. EL, Earlobe; T, tragus; S, SF, subcutaneous fat. (b) The SMAS is elevated with Kocher forceps. The parotid gland is observed in the sub-SMAS layer. P, Parotid gland; S, SMAS.
With respect to the relationship of the SMAS with mimetic muscles, Mitz and Peyronie2 reported that the SMAS invests in and extends into the external part of the superficial facial muscles involving the risorius, frontalis, platysma, and orbicularis oculi muscles. Stuzin et al7 reported that the SMAS invests in the zygomaticus major and zygomaticus minor, in addition to the muscles described by Mitz and Peyronie.2 The mimetic muscle layer is three-dimensional, and each of its muscles is located at a different depth from the surface. According to embryologic hypothesis, these facial muscles originate from three layers: the sphincter colli superficialis, sphincter colli profundus, and platysma, the last of which is located between the two sphincters. The sphincter colli profundus differentiates and becomes the buccinators, orbicularis oris, levator anguli oris, levator labii superioris, depressor anguli oris, and similar muscles. The platysma becomes other facial muscles, and the sphincter colli superficialis degenerates in many mammals. Freilinger et al8 reported the three-dimensional structure of the mimetic muscles as comprising four layers: layer 1, depressor anguli oris, zygomaticus minor, and orbicularis oculi; layer 2, depressor labii inferioris, risorius, platysma, zygomaticus major, and levator labii superioris alaeque nasi; layer 3, orbicularis oris and levator labii superioris; and layer 4, mentalis, levator anguli oris, and buccinator. The SMAS is presumed to have a close relationship with the two superficial layers of the mimetic muscles as described by Freilinger et al.8 According to Freilinger et al, however, some muscles are superficial to the SMAS (e.g., the platysma). Thus, the descriptions of the SMAS are presumed to be based more on clinical theory than strictly on embryologic theory.
There are many opinions about the embryologic origin of the SMAS.2,9 For example, some researchers have reported that the superficial fascia (tela subcutanea), which is a loose fibrous layer located just under the skin, is also observed in other parts of the body.2 Others have described fibrous degeneration of the platysma,5 a distinct fibromuscular layer comprising the platysma and parotid fascia,10 a musculoaponeurotic layer continuous with the platysma,6 and an evolutionary form of the panniculus carnosus.11 Some reports state that the SMAS contains muscle fibers,2,8 which indicates the embryologic origin of the SMAS layer. One anatomical textbook also shows that the platysma sometimes extends farther upward than usual, in some cases as high as the zygoma.12 Such a markedly upward-extending platysma is considered to represent remaining muscle fibers along the platysma layer. Another possibility is that a primitive muscle remains in the SMAS layer.13 Lei et al14 termed the muscle that spreads over the parotid gland the transverse nuchae muscle and assumed that this muscle is the SMAS muscle fiber described by Mitz and Peyronie.2 This muscle was found in about 5% of our dissections.
Histologic Findings of the SMAS
Parotid Area to Cheek Region
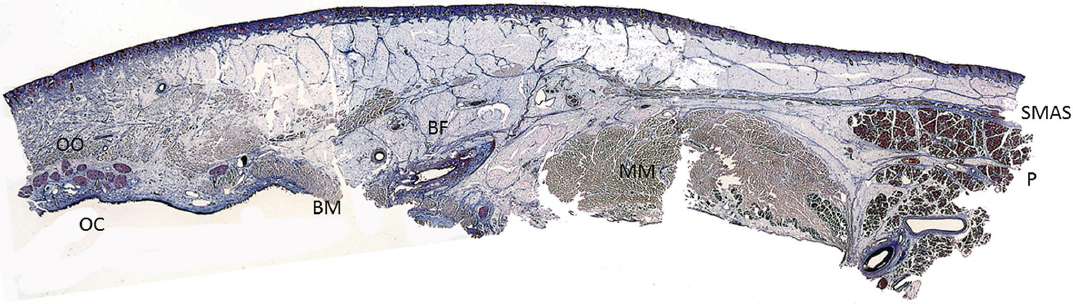
The SMAS is a thick membranous tissue that lies on the parotid gland and extends anteriorly, maintaining almost the same thickness until reaching the anterior border of the masseter (Fig. 11.2). Some branched muscular fibers of the platysma are present within the SMAS layer. The subcutaneous fat tissue layer is relatively thin in this area. The fibrous septa within this layer basically run parallel to the SMAS and delineate long, ovalshaped fat tissue in the horizontal plane. The SMAS becomes dramatically thinner beyond the anterior border of the masseter as it enters the cheek area; it can be barely traced by the position of split peripheral part of the platysma. The thick fat tissue superficial to the SMAS layer is the malar fat pad. This fat tissue contains fibrous septa that run perpendicular to the SMAS toward the dermis and separate the fat tissue into long ovals in the vertical plane. The fat tissue observed anterior to the masseter is the buccal fat pad, which fills the masticatory space.
Temporal Region
In the temporal region, the SMAS meets the superficial temporal fascia (Fig. 11.3). The superficial temporal fascia usually comprises fibrous tissue without muscle; however, it sometimes contains visible degenerative facial muscles such as the superior auricular muscle and temporoparietal muscle. The SMAS becomes somewhat ambiguous between these two fasciae, around the region of the zygomatic arch. Toward the temporal region, the SMAS layer separates into fibers containing fat tissue, no longer constituting a sheet of membrane. This finding is in contrast to the idea that the SMAS is continuous. The fibers gradually converge as they course upward. The subcutaneous fat layer above the SMAS also becomes thinner toward the head.
Lower Eyelid
It is generally recognized that the SMAS runs superficial to the zygomaticus major and minor and continues to the orbicularis oculi; however, it is difficult to confirm that the SMAS constitutes one continuous sheet in this area (Fig. 11.4). The thick fat tissue overlying the SMAS layer is the malar fat pad. It is thick in the middle region of the cheek and ends at the orbital rim. The fat pad is vertically long and oval in shape, and its fibrous septa are strongly connected as they course toward the dermis. The fat tissue beneath the orbicularis oculi is the suborbicularis oculi fat pad.
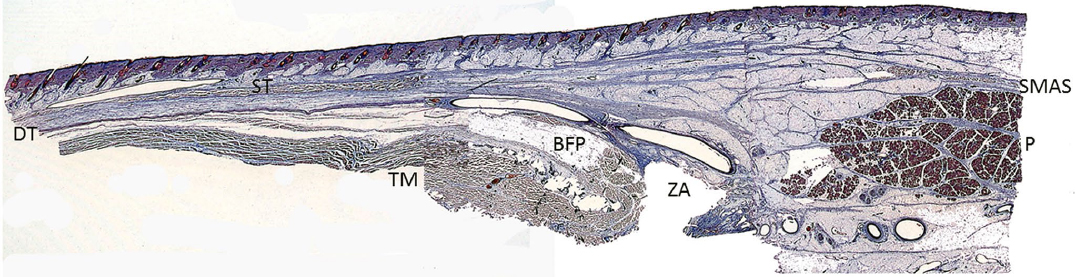
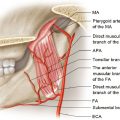
Fig. 11.3 Cross section from the parotid gland to the temporal region (composite photograph of three preparation specimens, Masson trichrome stain, ×1). BF, Buccal fat pad; DT, deep temporal fascia; P, parotid gland; SMAS, superficial musculoaponeurotic system; ST, superficial temporal fascia (in this case, the temporoparietal muscle); TM, temporalis muscle; ZA, zygomatic arch (removed).