Sun Reactions and Sun Protection
Fareesa Shuja
Zena W. Zoghbi
I. BACKGROUND
The sun radiates a broad system of energy that may be categorized in terms of the wavelength of its electromagnetic waves. The radiation reaching the earth’s surface may be subdivided into infrared (800 to 1,700 nm), visible (400 to 800 nm), and ultraviolet (290 to 400 nm). Ultraviolet radiation (UVR) can be further divided into three bands (Table 54-1).
Ultraviolet A (UVA) radiation (320 to 400 nm) causes immediate pigment darkening through distribution of preformed melanin, is carcinogenic, and suppresses the immune system.1 Ultraviolet B (UVB) radiation (290 to 320 nm) causes delayed pigment darkening, the result of DNA damage and a compensatory increase in melanogenesis.2 Chronic exposure to UVB is the most important factor in the development of skin cancers. Ultraviolet C (UVC) radiation (200 to 290 nm) is absorbed by the ozone layer and does not reach the earth’s surface. Though midday UVR is 10% UVB and 90% UVA, UVB is 1,000 times more erythemogenic than UVA, making it the major culprit in skin carcinogenesis.2 UVR induces genetic changes via chromosome damage and the inactivation of tumor suppressor genes such as p53. Skin types can be classified on the basis of response to UVR (Table 54-2).
II. CLINICAL PRESENTATION
A. Sunburn. Please see Chapter 42.
B. Indoor Tanning. The use of indoor tanning beds in the United States is a $3 billion per year industry.1 The sunlamps in these tanning units emit four times more UVA and two times more UVB than natural sunlight. This dose can produce erythema and melanogenesis but does not provide the protection of a naturally occurring tan, because there is no thickening of the stratum corneum nor is there an increase in the minimal erythema dose. The major concern regarding tanning beds is the carcinogenic effect of multiple doses of UVL.
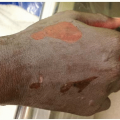
C. Dermatoheliosis. Photoaging, caused by chronic exposure to UVR, is due to alterations in the collagen and elastic fibers in the papillary dermis. It can manifest in a myriad of ways including Milian citrine skin (diffusely yellow hue), poikiloderma, cysts and comedones on the face (Favre-Racouchot syndrome), colloid milium, cutis rhomboidalis nuchae (leathery skin with exaggerated skin markings on the neck), elastotic nodules on the helices and forearms, actinic purpura, and stellate pseudoscars (Fig. 54-1).
D. Photosensitivity
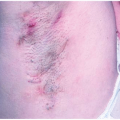
1. Photoallergy. Photoallergy requires prior sensitization, exposure to UVA light (UVB is less commonly implicated), and the administration of a photosensitizing systemic drug or an external contactant2 (Fig. 54-2). Clues to this diagnosis are medication history and the photodistribution of the skin findings (i.e., sparing of submental region). In a subset of patients, persistent photoallergy produces a chronic eczematous eruption, termed chronic actinic dermatitis, which persists even once the photosensitizer has been eliminated. These patients have broad-spectrum photosensitivity to both UVA and UVB light. Strict sun avoidance is key to treatment, though many patients also require systemic steroids or immunosuppressants.
TABLE 54-1 Ultraviolet Radiation Bands | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
TABLE 54-2 Skin Types | ||||
|---|---|---|---|---|
|