Chapter 37 Stryker Biosteon Cross-Pin Femoral Fixation for Soft-Tissue Anterior Cruciate Ligament Reconstruction
Introduction
In the past, soft-tissue anterior cruciate ligament (ACL) reconstructions have had several distinct disadvantages, despite the fact that multiple-strand hamstring grafts have been shown to have higher strength, stiffness, and cross-sectional area compared with patellar tendon grafts.1–3 Soft-tissue healing into bone tunnels is considerably slower than bone–bone healing (about three times slower4) and probably takes as long as 10 to 12 months for mature healing with Sharpey’s fibers to occur.5 Fixation points distant from the intraarticular portion of the graft have resulted in more motion of the graft within the tunnel, creating additional problems with graft–tunnel healing, as well as contributing to tunnel widening. Fixation has traditionally been the weak link in soft-tissue reconstructions, with constructs that both were weak initially and failed to withstand extended cyclical loading, which would be necessary to allow the additional time for soft-tissue–bone healing to occur. However, the morbidity of hamstring harvest seems to offer several significant advantages over that of patellar tendon grafts, including issues such as extensor weakness, anterior knee pain, patellar entrapment/patella baja, and patella fracture. In short, the conventional wisdom was that patellar tendon grafts provided tighter knees with more secondary problems, whereas hamstring grafts resulted in increased laxity but less morbidity.
Successful ACL reconstruction using hamstring autograft requires stable initial graft fixation and, ultimately, graft–bone healing. Hamstring reconstruction using femoral cross-pin fixation has been shown to have excellent initial mechanical properties, including pullout strength.8,9 Whereas femoral interference screw fixation requires a slightly more anterior femoral tunnel that fails to reproduce native ACL anatomy exactly, cross-pin fixation allows for placement of the femoral tunnel in the far posterolateral notch, a more anatomical position that provides improved biomechanical properties. The Stryker Biosteon Femoral Cross-Pin technique described in this chapter has the mechanical advantage of achieving “press-fit” graft fixation close to the knee joint and therefore increased graft stiffness,10 as well as the biological advantage of not interfering with bony and soft-tissue–bone healing.
Why Hydroxyapatite?
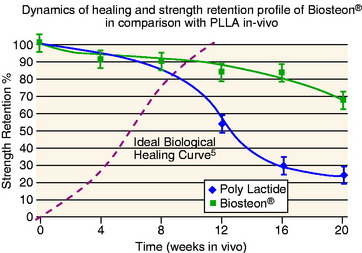
Hydroxyapatite has been widely investigated and used extensively as a bone graft substitute, and it has a track record of being safe and effective (references). The basic advantages of this application are: (1) pH buffering, (2) the implant material is replaced by bone, and (3) the modulus of elasticity is matched to bone (i.e., no stress shielding). In terms of pH, hydroxyapatite particles provide a buffering effect as the poly-L-lactic acid (PLLA) is degraded into lactic acid.11 The material is therefore not subject to autocatalytic degradation, which can result in formation of a sterile abscess. This also serves to create a more controlled degradation process, with more gradual loss of strength over an extended period of time compared with PLLA alone (Fig. 37-1).
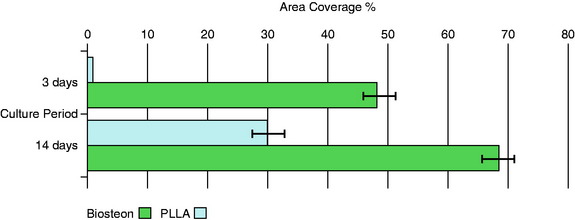
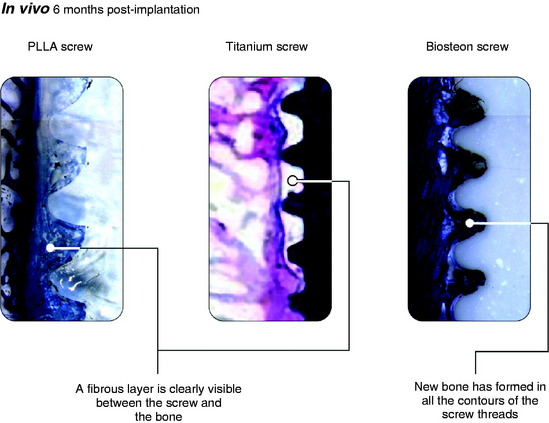
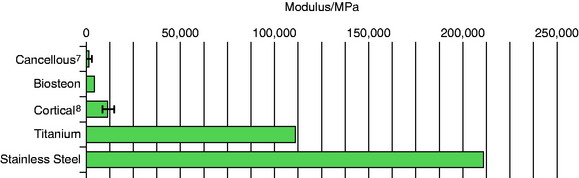
Osteoblasts bind preferentially to the surface of Biosteon as compared with poly-L-lactic acid (PLLA) alone (Fig. 37-2). Hydroxyapatite is remodeled through cell-mediated processes. Osteoblasts cultured on the surface of hydroxyapatite express genes associated with the production of osteocalcin and CBFA-1 (proteins involved in the process of osteogenesis). With hydroxyapatite, a direct biological bond is achieved through osteoconduction, with less of a fibrotic reaction. It is therefore less likely that fixation will be compromised by an interface consisting of fibrous tissue that encapsulates the implant (Fig. 37-3). As far as modulus of elasticity, Biosteon lies somewhere between the moduli of cortical and cancellous bone (Fig. 37-4), thereby greatly decreasing the risk of stress shielding, even prior to the breakdown of the implant material. In short, hydroxyapatite enhances the healing properties of PLLA while minimizing many of the drawbacks.
Surgical Technique
Initial Arthroscopy
The patient receives intravenous antibiotics preoperatively. After induction of anesthesia, an exam under anesthesia is performed. The patient is then positioned supine with the operative leg in an arthroscopic leg holder and a tourniquet on the upper thigh. The knee is routinely injected with 30 mL of 0.25% bupivacaine (Marcaine) at the beginning of the case for purposes of preemptive analgesia. Diagnostic arthroscopy is performed, and any chondral or meniscal procedures are performed at this time. A minimal lateral wall notchplasty is performed for visualization purposes only; we rely upon accurate graft placement rather than an aggressive notchplasty to avoid impingement, as a débrided notch has been shown to regrow.12 In addition, an overzealous notchplasty may have deleterious effects on the ACL reconstruction by altering the femoral attachment site and increasing graft forces, resulting in loosening.13,14 Furthermore, removal of too much of the lateral condyle can change joint contact forces significantly.15 Preservation of the integrity of the fat pad is also of paramount importance because it reduces the risk of patellar entrapment during recovery and rehabilitation.16,17 Placement of the anterolateral portal a few millimeters superior to the conventional position serves to avoid the fat pad and will improve visualization without the need to débride or excise any of the fat pad. We typically place the anterolateral portal at the level of the distal pole of the patella (if patella alta is not present), immediately lateral to the patellar tendon.
Femoral Tunnel Location and Preparation
Related posts:
 Anatomical Anterior Cruciate Ligament Reconstruction with Double-Bundle, Double-Stranded Hamstring Autografts: A Four-Tunnel Technique
Anatomical Anterior Cruciate Ligament Reconstruction with Double-Bundle, Double-Stranded Hamstring Autografts: A Four-Tunnel Technique
 Tibial Fixation for Anterior Cruciate Ligament Hamstring Grafts: 10 Techniques that Improve Fixation
Tibial Fixation for Anterior Cruciate Ligament Hamstring Grafts: 10 Techniques that Improve Fixation
 Hamstring Regeneration Following Harvest for Anterior Cruciate Ligament Reconstruction: A Review of the Current Literature
Hamstring Regeneration Following Harvest for Anterior Cruciate Ligament Reconstruction: A Review of the Current Literature
 Revision Anterior Cruciate Ligament Reconstruction Using Autologous Hamstring Tendons
Revision Anterior Cruciate Ligament Reconstruction Using Autologous Hamstring Tendons
 High-Stiffness, Slippage-Resistant Cortical Fixation Has Many Advantages over Intratunnel Fixation
High-Stiffness, Slippage-Resistant Cortical Fixation Has Many Advantages over Intratunnel Fixation
 Endobutton Anterior Cruciate Ligament Reconstruction Femoral Fixation
Endobutton Anterior Cruciate Ligament Reconstruction Femoral Fixation
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


