Stereotactically Guided Breast Percutaneous Needle Biopsy
Arthur G. Lerner
Introduction
History of Stereotactic Breast Biopsies
Stereotactic breast biopsies were first discussed in 1977 (1). Dr. Kambiz Dowlatshahi, a surgeon at Rush Presbyterian Medical College in Chicago, Illinois, brought the first prone stereotactic table to the United States in the mid-1980s. After learning this technology at the Karolinska Institute in Germany, Dr. Dowlatshahi performed the first stereotactic breast biopsy in 1987 (2) (Fig. 4.1). Since that time, there have been many significant changes in the stereotactic technology and in the biopsy techniques and devices employed during these interventions.
Initially, the prone stereotactic technology was an analog imaging system. The determination of the location of the image abnormality was accomplished using a digitizer. By placing marks on the mammogram films with a T square, measurements were taken and the co-ordinates of the lesion were determined and entered into the system by hand, using a set of micrometer dials. Today, the system is completely digital, and the determination of the co-ordinates of the mammographic abnormality is made electronically from the digital images. This work is done at the imaging console (Fig. 4.2). The data points are entered into the system electronically without having to manually place the co-ordinates into the table’s database.
Another significant improvement in the biopsy methodology has been the evolution of the biopsy devices (3,4). In the early 1990s, spring-loaded core needles were developed to replace the fine needle aspiration (FNA) technique. The early core needle devices were 16 to 18 gauge, and eventually 14-gauge devices became the standard (Fig. 4.3). Large core, rotating cutter, vacuum-assisted biopsy devices have replaced the spring-loaded 14-gauge core needles (Figs. 4.4–4.9). Radiofrequency devices are also in use and have the potential to remove the entire imaging abnormality in a single intact specimen (Figs. 4.10 and 4.11). These new tools represent a significant change in biopsy devices from the original FNA technology first employed on the stereotactic table. The
result has been a decrease in the nondiagnostic and false-negative biopsies as a result of the larger samples these devices provide for pathologic analysis.
result has been a decrease in the nondiagnostic and false-negative biopsies as a result of the larger samples these devices provide for pathologic analysis.
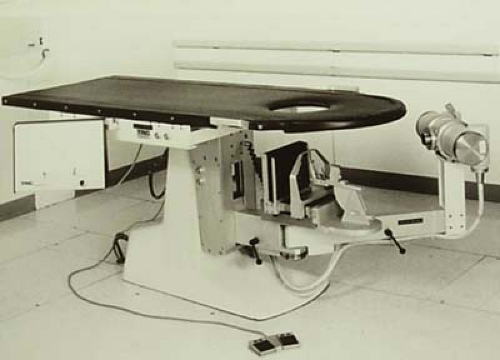 Figure 4.1 The first stereotactic biopsy in the United States was performed by Dr. Kambiz Dowlatshahi in 1987 on this table. Dr. Dowlatshahi brought this table from Germany where he learned the technology. (Photograph reprinted with the permission of Dr. Dowlatshahi.) |
 Figure 4.2 Computer station for image viewing, targeting of the lesion, and transmission of the data electronically to the table. |
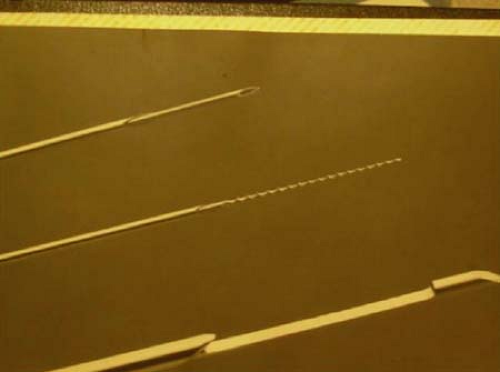 Figure 4.3 Tissue sampling was initially performed with a fine needle aspiration cytology technique. (Photograph reprinted with the permission of Dr. Kambiz Dowlatshahi.) |
 Figure 4.4 The first early spring-loaded core needles used on the prone stereotactic table. |
 Figure 4.5 The first vacuum-assisted biopsy device was manufactured by Biopysis. This product was eventually bought by Ethicon Endo-Surgery and manufactured and sold as Mammotome. |
 Figure 4.6 Encore vacuum-assisted biopsy device by SenoRx. |
 Figure 4.7 The ATEC vacuum-assisted biopsy device manufactured by Suros, Inc. |
 Figure 4.8 Vacuum-assisted multiple insertion biopsy device manufactured by Bard Inc. |
 Figure 4.9 Large core biopsy needle from Site Select. This rotating cutter needle cores a single large sample to include the targeted lesion. |
 Figure 4.10 Radiofrequency biopsy needle manufactured by Rubicor. It has a loop and a bag that is deployed and rotated around the target. The loop is energized and cuts the tissue, which is captured in the bag and extracted from the breast. |
 Figure 4.11 In Tact, a radiofrequency device that has an energized basket at the tip of the device that surrounds the target when deployed. The energized basket arms cut the tissue, and once the tissue is secured in the basket, the device is removed from the breast with a single sample of tissue that includes the targeted lesion. |
 Figure 4.12 The original Fischer Mammotest system with the table, workstation, and x-ray generator. This is a unidirectional table. The patient is always facing the same way once in the prone position on the table. The C arm rotates through a 270-degree arc, allowing all approaches to the breast except a caudal to cranial approach. |
Presently, almost all diagnostic breast biopsies can be accomplished with a needle rather than with a knife (5).
The Technology
There are two different targeting systems employed in the stereotactic technology (6,7). The table originally developed by Fischer Imaging of Denver Co. (Fig. 4.12) utilizes a polar co-ordinating system, where the co-ordinates of the indexed mammographic lesion are defined by the distances from a fixed point and angular distances from a reference line. The horizontal and vertical co-ordinates are expressed in degrees, while the depth to the center of the lesion is given in millimeters.
On the Lorad Multicare table (Fig. 4.13), a Cartesian co-ordinating system is used. Here, distances are determined from a reference point, where the horizontal, vertical, and depth axes intersect at right angles and define the target. Utilizing this system, all co-ordinates are given in millimeters.
A third prone table technology made by Giotto, in use at this time mainly in Europe, also utilizes a Cartesian targeting system, incorporated into a mammography unit with patient positioning on a prone table.
There are numerous “add-on” or upright systems, where a targeting and biopsy technology is added to an existing mammography unit, and the targeting and biopsy are done with the patient either upright or lying on her side (Fig. 4.14). These add-on systems allow the mammography unit to be used for screening or diagnostic mammography when biopsies are not being performed. This differs from the prone systems, which are only for stereotactic procedures and not applicable to standard mammography.
The advantages of the prone tables are the ability to biopsy the lesion in the breast from multiple approaches, where on the upright systems the approaches are somewhat limited.
There are more patient issues reported with the “add-on” systems, particularly vasovagal reactions. These upright systems do, however, allow access to lesions close to the chest without needing exaggerated positioning that may be necessary on the prone tables.
There are more patient issues reported with the “add-on” systems, particularly vasovagal reactions. These upright systems do, however, allow access to lesions close to the chest without needing exaggerated positioning that may be necessary on the prone tables.
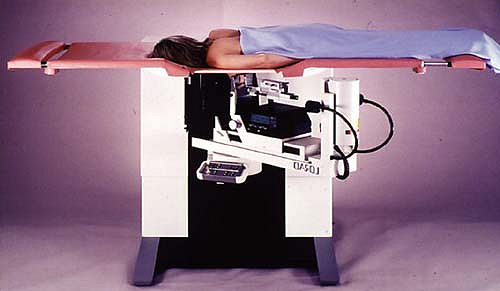 Figure 4.13 The Lorad Multicare prone stereotactic table. This is a bidirectional table. The patient can be positioned in either direction, allowing any approach to either breast. |
Related posts:
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


