Fig. 4.1
‘Double-bladed’ reciprocating saws used in reduction malarplasty (a). The width between the blades may vary, ranging from 2 to 7 mm. The saws are used for precise and equal bone resection in the zygomatic body region (coloured in red) during an L-shaped osteotomy (b)
Secondly, the amount of posterior setback of the zygomatic body should be decided. Usually, the point that indicates the maximum malar projection is anterolaterally malpositioned in patients with a prominent zygoma [3]. Accordingly, not only a medial repositioning of the zygomatic body but also a posterior setback should be done together when correcting a projecting zygomatic bone. During this step, pre-bent titanium plates may be used to precisely perform the setback procedure. The size of the step (i.e. the amount of bending) in each plate ranges from 0 to 5 mm (Fig. 4.2). If the projection of the zygomatic bone is more extensive, a pre-bent plate with a larger-sized step should be used and vice versa. By using these pre-bent titanium plates, it is easier to equally reposition the zygomatic body in cases with a symmetric feature. Also in asymmetric cases, it is easier to correct the asymmetry by using different sized plates and differentially reposition the zygomatic body.
Fig. 4.2
Pre-bent titanium plates used in reduction malarplasty. The three-hole plates are used for fixation of the zygomatic arch, and the six-hole plates are used for the zygomatic body. Different sizes are available for rigid and accurate bone repositioning
The third factor that should be determined during a reduction malarplasty is the amount of medial repositioning of the zygomatic arch. Most of the patients with a prominent zygoma also have a prominence in the arch region that should be repositioned inwardly to reduce the outward projection. As mentioned above, the zygomatic arch is cut through an incision in the sideburn. Then, the arch portion anterior to the osteotomy site is pushed inwardly and rigidly fixed. The amount of medial repositioning required can be precisely achieved using a linear three-hole pre-bent titanium plate. The step size of these plates ranges from 0 to 4 mm; choice of plate depends on the lateral prominence of the arch region (Fig. 4.2).
Mandible Reduction
The conventional mandible angle reduction technique involves an oscillating saw through an intraoral approach [9–11]. However, before carrying out the main osteotomy procedure, a ‘guarded’ oscillating saw can be used to mark the proposed osteotomy line [1, 12, 13]. The guarded saw which has a small oscillating saw blade that is shielded at different distances of 2, 3, 4, 5 or 6 mm (Fig. 4.3). Size of the guarded saw to be used is determined by considering the amount of resection that should be done in the mandibular body and the path of the inferior alveolar nerve (i.e. the distance between the lower mandible border and the route of the nerve). By using these guarded oscillating saws, it is possible to perform the bony resection precisely in a more uniform fashion. More importantly, by using a guarded saw, unintentional over-resection can be avoided, and the possibility of a nerve injury can be decreased. Furthermore, in cases with pre-existing jawline asymmetry, bone resection can be differentially carried out using different-sized guarded saws. After the osteotomy is initiated with a guarded saw, larger oscillating saws are serially used to complete the bone resection.
Fig. 4.3
‘Guarded’ oscillating saws used in mandibular angloplasty (a). Each saw has a small oscillating saw that is shielded at various distances. The saw guides precise bone resection in the mandibular body region (coloured in red) while avoiding over-resection and nerve injury (b)
Genioplasty
Genioplasty is decidedly the most versatile and practical surgical tool in the field of facial bone surgery. Genioplasty can be done in an isolated manner or, more frequently, in combination with other facial bone surgeries such as orthognathic surgery or facial bone contouring surgery [14]. For example, genioplasty can be carried out independently in patients with either a small and weak chin or a protruding chin by repositioning the chin in an anteroposterior dimension [15, 16]. If a patient has a disproportionately short lower face, elongation of the chin may be needed in addition to shortening of the lower face [12, 15]. Genioplasty can also be done as a part of a chin narrowing procedure [13, 17].
When a bone resection is required, for example, during a chin narrowing or vertical shortening procedure, the abovementioned double-bladed reciprocating saw can be used for a precise and equal osteotomy (Fig. 4.4) [1]. When planning a chin advancement or setback, a pre-bent plate can be used to precisely control the amount of anteroposterior adjustments, each plate differing in size by steps from 0 to 10 mm (Fig. 4.5). The plate that is used should be selected based on preoperative cephalometric analysis [14, 15]. By using pre-bent plates, the exact amount of chin advancement or setback determined preoperatively can be achieved.
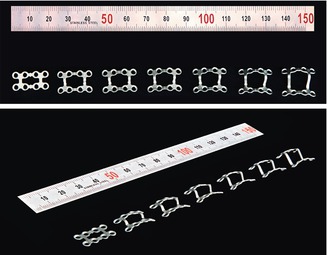
Fig. 4.4
A double-bladed reciprocating saw used in genioplasty. During a chin narrowing or vertical shortening procedure, the saw can be used for precise and equal bone resection (coloured in red)
Fig. 4.5
Pre-bent titanium plates used in genioplasty. The plates are used for controlling the degree of anteroposterior adjustment during chin advancement or setback in accordance with preoperative measures
Discussion
Complications in facial bone contouring surgery may occur either due to errors in judgment during patient evaluation or during the operative procedures [1]. Standard surgical techniques and instruments that are described here can be used to avoid unfavourable outcomes due to operative technical errors. Possible complications after facial bone surgery include oedema, haematoma and infection. In addition to these general complications, soft-tissue sagging, transient sensory disturbance, asymmetry and under-correction or overcorrection of zygoma contours are relatively common complications that occur after a reduction malarplasty [4]. Double-bladed reciprocating saws are used to make osteotomies more accurate and predictable. This can decrease postoperative asymmetry and the possibility of under- or overcorrection. Furthermore, by using different-sized double-bladed saws on each side, the surgeon can precisely correct pre-existing asymmetry. While rigid osteofixation is essential to achieve complete bone union and reduce soft-tissue sagging, the use of pre-bent plates on both the zygomatic body and arch allows more precise repositioning [1, 3, 6]. Comparing the incidence of complications with previous studies using the proposed surgical instruments, or not, resulted in a lower incidence of postoperative asymmetry (0.8% versus 2.9%) and overcorrection (0.4% versus 0.6%) [1, 2, 18]. Also, the incidence of neurosensory deficit was markedly lower compared in studies which the same intraoral and sideburn approach and L-shaped osteotomy was used for reduction malarplasty (6.7% versus 9.4%) [1, 2, 4].
Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


