Soft Tissue Flaps for Maxillary Reconstruction
Ahmed M. Hashem
Brian R. Gastman
DEFINITION
Maxillary reconstruction is the process of rebuilding and coverage of midface and cheek defects.
Tissue loss often results from oncologic resections but can also occur secondary to blunt or penetrating trauma and, less commonly, from necrotizing infections.
The loss of critical soft tissue components such as the lower eyelid, the nose, the upper lip, and oral commissure adds significant complexity to the reconstruction.
The functional implications involve speech, mastication, and deglutition.
ANATOMY
The maxilla is a complex structure occupying the midface.
Conceptually, it is a six-walled construct (hexahedron) bounded by the orbit superiorly, the palate and oral cavity inferiorly, the nasal airway medially, and the infratemporal fossa and cranial base posteriorly.
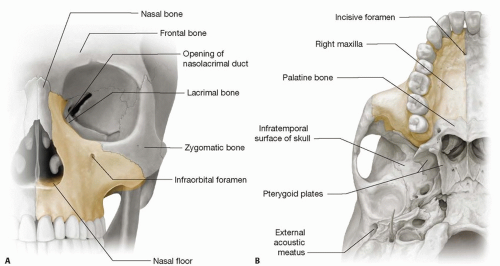
FIG 1 • A. Left maxilla (frontal view). Bony articulations of the maxilla. The maxilla shares in the formation of the orbital floor and forms the lateral nasal wall. B. Right maxilla (inferior view). The maxilla forms the roof of the mouth (the palate) and is related posteriorly to the infratemporal fossa and cranial base.
The maxillary sinus is a mucosa-lined air cavity in the maxillary process that drains into the middle meatus of the nose.
The sinus is rudimentary at birth but undergoes rapid expansion 6 to 7 years after puberty.
The skeletal framework consists mainly of the maxillary and zygomatic bones, which articulate with parts of the pterygoid, palatine, lacrimal, ethmoid, and sphenoid bones (see FIG 1A).
The vertical maxillary buttresses and the horizontally oriented alveolar process define the contour of the midface, contribute to vertical facial height, carry the dental elements of the upper jaw, and support the upper lip.1
The soft tissues comprising the skin, lining mucosa, and intervening facial musculature constitute the lower eyelid, the cheek, the upper lip, and oral commissure.1
From a reconstructive standpoint, it is critical to appreciate that the maxilla forms the floor of the orbit, the roof of the mouth (the palate), and the lateral nasal wall including the lacrimal system.1
From a functional perspective, its integrity is critical for normal speech, mastication, and deglutition.1
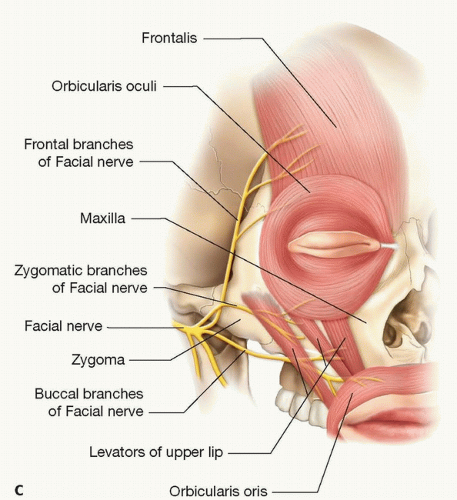
FIG 1 (Continued) • C. Right maxilla. The maxilla is related to the critical facial muscles (orbicularis oculi, orbicularis oris, levators of the upper lip) and the frontal, zygomatic, and buccal rami of the facial nerve.
Anteriorly, it is related to the facial and angular arteries, whereas posteriorly, it is in close proximity to the internal maxillary artery, the pterygoid venous plexus, and the last four cranial nerves.
The zygomatic and buccal branches of the facial nerve ramify in the sub-SMAS plane of the cheek to supply the orbicularis oculi, the orbicularis oris, and the levators of the upper lip (FIG 1C).
The infraorbital nerve travels in the floor of the orbit to emerge on the cheek through the infraorbital foramen and provide sensation to the midface. The zygomaticofacial nerve also appears anteriorly through a foramen inferior to the lateral part of the inferior orbital rim.
PATHOGENESIS
Maxillary defects occur in many cases secondary to tumor extirpation of malignancies originating in the paranasal sinuses, the nasal cavity, the palate, or the orbit.
In other cases, aggressive malignancies arising from the intraoral mucosa, the cheek skin, or the salivary glands may invade the maxilla and require extensive composite tissue excisions.1
High-energy traumatic injuries (eg, gunshot wounds) constitute another cause of challenging maxillary defects.2
Necrotizing inflammations like noma (cancrum oris)3 and malignant pyoderma in association with granulomatosis with polyangiitis have also been described.4
Composite resections where lining, support, and external skin are missing can pose a significant reconstructive challenge.
PATIENT HISTORY AND PHYSICAL FINDINGS
A complete history should be obtained to identify comorbid conditions that may be optimized preoperatively.
A personal or family history of clotting/bleeding abnormalities should be elicited.
History of prior surgery, neck dissection, or radiation therapy of the head and neck should be noted.
Physical examination of the head and neck should evaluate dentition, speech and swallowing, facial nerve function, and sensory innervation.
Changes in skin texture and quality, eyelid function and support, and mouth opening should be assessed.
The expected resection should be envisioned and soft tissue and bony requirements estimated. Close collaboration with the ablative surgeon is crucial in this regard.
Assessment of potential local and distant tissue donor sites should be undertaken (eg, temporalis, pectoralis major, radial forearm, rectus abdominis, anterolateral thigh [ALT] flap).
Allen test is useful for evaluation of the palmar arch in patients who may require a radial forearm flap.
Assessment of soft tissue thickness and previous scars/surgery is important to identify first-line and second-line choices for reconstruction.
IMAGING
Imaging modalities like CT scan and MRI are useful preoperatively to determine the size and extent of the tumor and understand the potential resulting defect. These studies are also useful in patients with acquired defects of the maxilla resulting from trauma or infections.
A 3D CT scan helps with preoperative virtual surgical planning and manufacturing of custom-designed models, templates, osteotomy guides, and prebent plates and selection of optimum screw size and site especially if dentoalveolar reconstruction and functional occlusion are contemplated. However, these options are most useful for osseous reconstruction of maxillary defects.
Duplex examination or CT angiography with 3D reconstruction is occasionally required to evaluate the neck vessels in difficult cases with prior neck dissection or radiotherapy.
Postoperatively, positron emission tomography (PET) and CT scan will be of benefit to assess the operative bed for tumor recurrence if a free flap was employed.
NONOPERATIVE MANAGEMENT
Custom-made obturators can be used to manage maxillary defects and can provide support for facial structures and separate the oral cavity from the maxillary sinus.
Obturators restore intelligible speech, prevent nasal regurge, and provide aesthetic contours.
Obturators maybe useful in patients at high risk for complex reconstructive procedures or, on occasion, as salvage of a failed reconstruction.
They may also be useful for small defects of the palate (<50% of the hard palate), providing rapid rehabilitation with no donor-site morbidity.
In general, obturators are best for small defects in the hard palate and are more difficult to secure in larger defects that involve the hard and soft palate.
The use of an obturator requires close preoperative, intraoperative, and postoperative collaboration between the oncologic surgeon, reconstructive team, and a prosthodontist. The steps necessary for obturator creation include:
Fabrication of dental casts, analysis of occlusion, and preoperative modeling
Creation of a temporary obturator manufactured from heat-processed polymethylmethacrylate, which is strong enough to provide a stable and functioning construct but is still adjustable intraoperatively using a bur or drill to fit the surgical defect
Split-thickness skin grafting of the buccal surface of the cheek flap and bolstering with the temporary obturator, which is fixed with screws or wires
Postoperative evaluation and adjustments
Fabrication of a permanent prosthesis fashioned from durable cast metal base (eg, titanium) after maturation of the surgical cavity and conclusion of radiotherapy
Use of obturators carries the advantage of visual inspection of the surgical site for tumor recurrence. This benefit, however, remains theoretical because reoperation is infrequent and modern imaging enables early detection. Nevertheless, many patients have been successfully served with these devices.
Disadvantages of obturators include leakage and nasal regurgitation due to imperfect fitting, the need for frequent cleaning and successive refinements as the tissues remodel.
SURGICAL MANAGEMENT
The development of microsurgical techniques enabled successful autogenous tissue reconstruction of complex maxillary and midface defects.
The approach is largely dictated by the extent of the defect and the functional requirements.
Simple defects can be closed with local soft tissue flaps and bone grafts when necessary and rarely pose a problem.
Complex composite defects involving external skin cover, structural support, and lining require planning for restoration of orbital floor support, lining of the nasal airway, palatal reconstruction, and resurfacing of surface defects that may include the upper lips, eyelids, and nose. In addition, dental restoration is necessary in most maxillary resections that involve the hard palate.
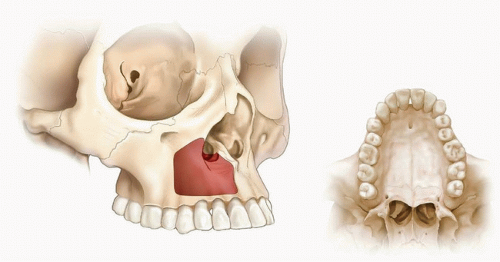
FIG 2 • In a type I (limited maxillectomy) defect, the anterior and medial walls are missing and occasionally the orbital floor; the palate is intact.
In this context, the classification system described by Cordeiro and Santamaria1 is useful to stratify maxillary/midface defects and evaluate their functional requirements. The resultant analysis is able to guide appropriate treatment strategies.1 Based on this schema, maxillectomy/midface defects can be categorized as follows:
Type I defect (limited maxillectomy): Only one or two walls—excluding the palate—of the hexahedron are missing. Usually, there is an absence of the anterior wall in conjunction with either the medial wall or the floor of the orbit (FIG 2).1
Type II defect (subtotal maxillectomy): The whole lower maxilla is absent (the dentoalveolar arch, the anterior, medial, and lateral walls, in addition to the palate), while the orbital floor is intact.
These are further subdivided into type II-A when less than half of the transverse hard palate is missing and type II-B when more than half of the transverse hard palate is resected (FIG 3).
Type III defect (total maxillectomy): The whole maxilla including the orbital floor is deficient. Type III defects are additionally split into type III-A if the orbital contents are preserved and type III-B if they are exenterated (extended maxillectomy) (FIG 4).1
The advent of vascularized composite allotransplantation (ie, facial transplantation) refined midface and maxillary reconstruction by replacing “like” with “exact like,” thus achieving a closer aesthetic match in terms of soft tissue and skeletal components.
The risks of lifelong immunosuppression nevertheless limit the use of this modality, which is still considered experimental, to a highly select group of patients (eg, trauma).
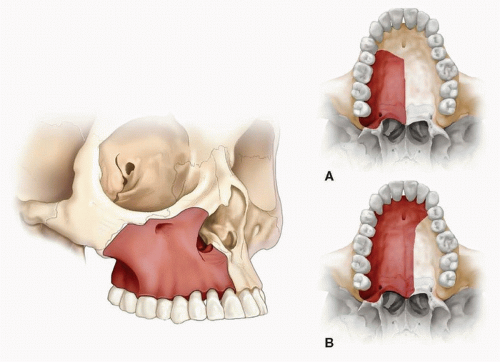 FIG 3 • Type II (subtotal maxillectomy) defect involves the lower maxilla including the palate. In type II-A, less than half of the transverse palate is missing. In type II-B, more than half of the transverse palate is resected. |
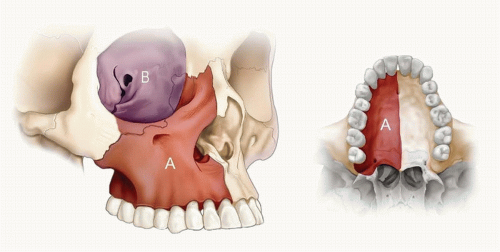 FIG 4 • Type III (total maxillectomy) defect. In type III-A, orbital contents are preserved. Type III-B is associated with orbital exenteration (extended maxillectomy). |
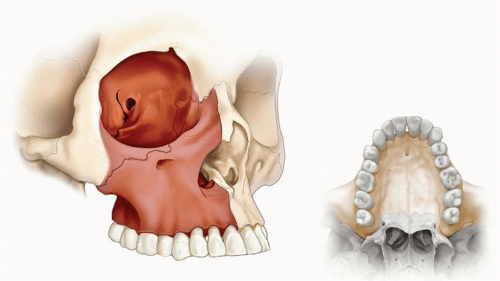 FIG 5 • In a type IV (orbitomaxillectomy) defect, the upper maxilla and orbit are missing, while the palate is intact. |
Preoperative Planning
Oncologic resections are by far the most common cause of maxillary defects. Consequently, adequate tumor clearance and tumor-free margins assume the highest priority in management. Close collaboration with the ablative surgeon is thus critical.
Resections may involve functional impairment of speech and oral intake in addition to loss of globe support and eyelid cover.
The reconstruction is best accomplished in a multidisciplinary setting with input from surgical oncology, medical oncology, radiotherapy, speech, nutrition, ophthalmology, and dentistry, in addition to reconstructive surgery.
Complex defects are often composite and require threedimensional planning to reconstruct lining, cover, and provide structural support. Accurate analysis of the functional needs is hence crucial. Accordingly, precise assessment of the extent of prospective resection based on clinical and imaging data should be undertaken.
Adjacent critical soft tissue components including the eye, lip, oral commissure, and nose are evaluated.
The neck is examined for previous scars and the availability of ipsilateral suitable recipient vessels.Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree