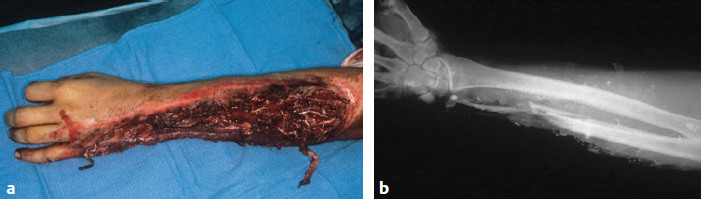
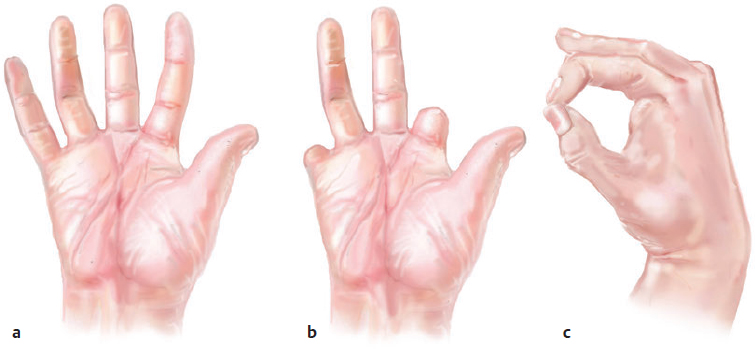
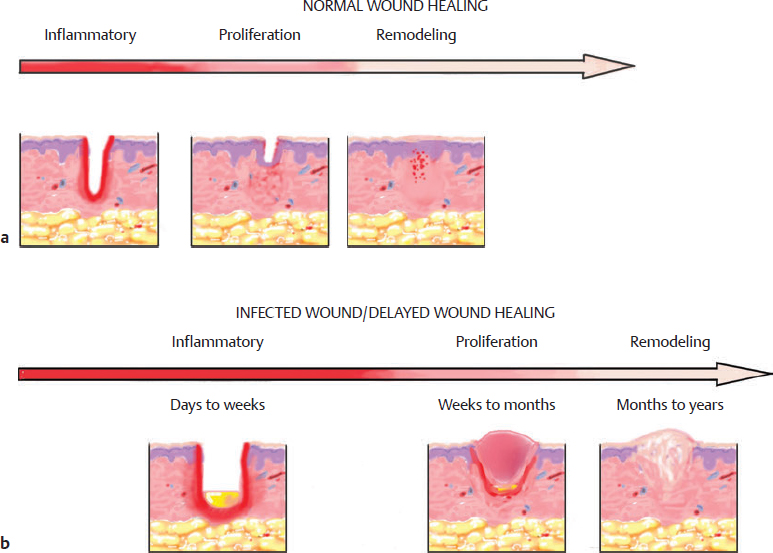
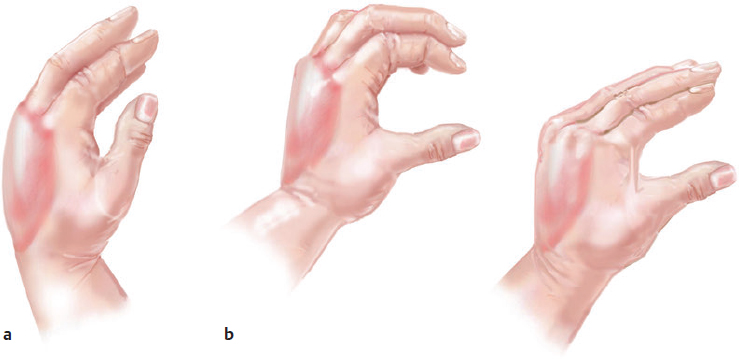
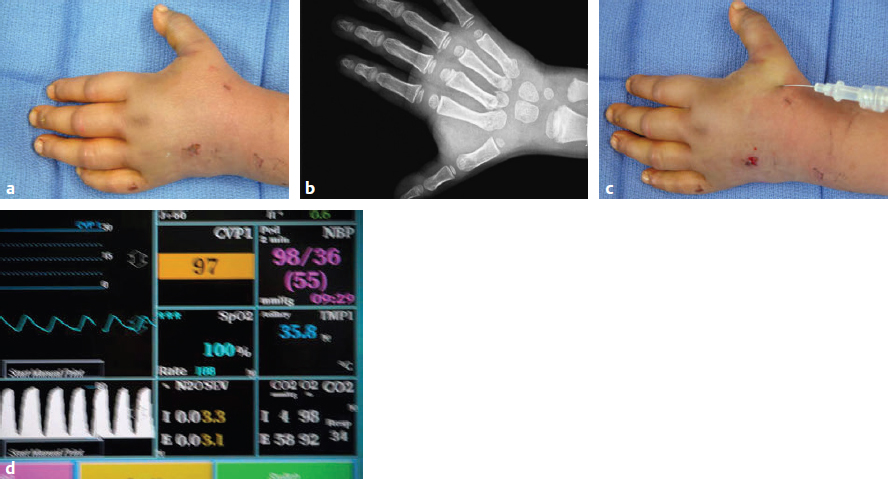
CHAPTER Mutilating upper extremity injuries generally cause substantial damage to more than one of the five basic tissues of the hand: integument, skeletal, vessels, nerves, and tendons.1 Injury to the hand and the subsequent healing process jeopardizes hand function, which depends on the intricate anatomical arrangements of these structures. Understanding the physiology of wound healing and the scarring process is crucial to restoring optimal functional outcome. Wound healing is the body’s response to injury. This complex process is divided into three distinct but overlapping phases: inflammation, proliferation, and remodeling.2 Immediately after injury, vasoconstriction and recruitment of platelets promote hemostasis. Platelets are activated to release neutrophils and macrophages, which both function in phagocytosis of microbes and debris. In the presence of foreign material or necrotic tissue, inflammatory mediators will persist, resulting in a prolonged inflammatory phase and delayed healing (Fig. 64.1). Early and meticulous débridement of nonviable, contaminated tissue is therefore essential to shorten the inflammatory phase and reduce edema. The proliferative phase overlaps with the ending of the inflammatory phase and consists of granulation tissue formation, neovascularization, reepithelialization, and extracellular matrix production. Fibroblasts migrate to the wound around day 3 and are primarily responsible for production of the structural proteins and collagen. The remodeling phase involves rearrangement of the collagen fibers to increase tensile strength of the wound. As the phases of wound healing progress, granulation tissue and collagen fibers form what will ultimately evolve into a scar. Reepithelialization and wound contraction have a crucial impact on scar formation. Epithelial cells from wound margins and residual dermal appendages within the wound bed migrate inward to fill the defect.2 Small wounds that are approximated early after injury heal rapidly without the need for significant wound volume reduction. This is healing by primary intention. Large wounds with significant tissue loss heal by secondary intention. There is gradual filling of the defect with granulation tissue, wound contraction, and reepithelialization at the wound edges. If an open wound overlying joints and tendons is allowed to heal by secondary intention, joint stiffness and deforming joint contracture may result. Early soft tissue coverage, when feasible, is a primary objective to avoid pathologic contractures. The cellular response to injury results in edema formation. The body sends fluids containing inflammatory cells, plasma proteins, and antibodies to the wound site after injury. In the injured hand, edema accumulates on the dorsum where there is dependent space, drawing the wrist into flexion, the metacarpophalangeal (MCP) joints hydraulically into extension, the proximal interphalangeal (IP) joints into flexion, and the thumb into adduction3 (Fig. 64.2). Therefore the traumatized hand must be immobilized in the intrinsic plus position with the MCP joints in flexion and the IP joints in extension. Early mobilization is emphasized, however, because it is necessary to reduce edema and preserve the gliding function of tissues. Peacock and Van Winkle4 described the concept of “one wound–one scar,” in which scar forms from the skin down through bone and binds together all surrounding tissues. Fundamental hand function, such as prehension, is restricted by the inability of the tissues to glide against each other. This concept forms the biologic basis for remodeling of the scar tissue. Secondary procedures after reconstruction of the injured hand such as tenolysis, joint contracture releases, or web space deepening may be necessary to improve mobility and function5 (Fig. 64.3). Fig. 64.1 (a) Normal timing of wound healing. The inflammatory phase occurs immediately after the injury and lasts approximately 4 to 6 days. The proliferative phase occurs at the termination of the inflammatory phase and lasts about 3 weeks. The remodeling phase begins at the fourth week and can last months to even years. (b) Delayed wound healing. In the presence of a contaminated wound, the inflammatory phase can persist for days to weeks if not adequately débrided. This in turn will postpone the start of the proliferative phase and delay wound healing. Fig. 64.2 (a) Injured hand position. Edema accumulates in the dorsum of the injured hand, which draws the wrist into flexion, the metacarpophalangeal (MCP) joints into hyperextension, the proximal interphalangeal joints into flexion, and the thumb into adduction. Additionally, the MCP joints are at their most voluminous in extension. The fluid-filled MCP joints hydraulically drive these joints into extension. (b) Intrinsic plus position. The traumatized hand must be appropriately immobilized with the MCP joints in flexion, the IP joints in extension, and the thumb in abduction to minimize joint stiffness. Fig. 64.3 (a) A 20-year-old man experienced a table saw injury to his nondominant hand that traversed through the metacarpophalangeal joints of the index to little fingers. Joint, tendon, and microvascular repairs were performed, but he had limited range of motion postoperatively. (b) The patient has flexion of all his fingers after dorsal MCP joint capsulotomies. (c) The patient has achieved extension of all his fingers after intrinsic muscle releases. Having the concept of wound healing and scar formation in mind throughout the reconstructive and repair process will help the surgeon to avoid common complications that result from mutilating hand injuries. This chapter describes the management of complex hand injuries and how to avoid unfavorable results at each stage. It explains how to address these complications and provides case illustrations. Because mutilating hand injuries often occur from high-impact mechanisms, patients may have sustained injuries to other organ systems that may be life-threatening. The standard advanced trauma life support protocol should be initiated to stabilize the patient before eliciting a thorough history and evaluation of the injured extremity. Partington et al6 studied the incidence of unrecognized injuries in patients referred for emergency microsurgery over a 7-year period. They found that 9 out of 1,100 patients (0.8%) transferred had unrecognized coexisting injuries that put the patient at high risk for morbidity and altered the original plan of care. Although the hand mutilation may be severe, it is rarely life-threatening; hence the mantra of “life before limb” should be abided before considering any reconstruction. A detailed history of the mechanism, timing, and location of injury will avoid underestimating the severity of injury and guide further management. The mechanism of injury can reveal the force and zone of injury. In the case of motor vehicle accidents, a high-speed rollover accident in which the patient was ejected from the vehicle will have a broader zone of injury requiring repair of multiple tissue layers. The time of injury and the time elapsed between injury and presentation is critically important, especially with a devascularizing injury. Warm ischemia for longer than 6 hours may affect successful digit replantation or revascularization. Delays longer than 6 to 12 hours may preclude primary closure because of a greater risk of infection. The environment of the injury is pertinent because the exposure to caustic industrial chemicals or highly contaminated farming fields will likely require more extensive and serial débridement (Fig. 64.4). Summary Box Common Complications, Causes, and Treatment Common Complications • Wound infection and dehiscence • Wound contraction and pathologic contractures • Tendon adhesion and joint contracture • Donor site morbidity and unaesthetic reconstruction • Dysesthetic and anesthetic hand • Nonunion and malunion Causes of Complications • Missed diagnosis and delayed treatment • Inadequate débridement • Poor planning • Poor skeletal fixation • Inadequate soft tissue coverage • Excessively delayed soft tissue coverage • Improper splinting and edema management • Improper timing of nerve and tendon repair Treatment of Complications • “Re-creating” the original wound for soft tissue coverage when the initial procedure was inadequate • Bone grafting and osteotomies for bone malunion and nonunion • Joint releases • Tenolysis • Neurolysis and neuroma excision Other important aspects of the history that should not be missed include the patient’s overall functional status, comorbidities, and occupational goals, because this information will help to formulate a treatment plan. Elderly patients with cardiovascular or pulmonary disease have increased perioperative morbidity and may benefit from shorter, simplified reconstruction. Smoking and use of vasoactive drugs have a deleterious effect on microcirculation and are often a contraindication to complex microvascular reconstruction.1 The patient’s occupation, preinjury functional status, and willingness to adhere to a rehabilitation program are also relevant factors. For instance, a self-employed construction worker will likely be interested in a procedure that offers expeditious return to work, whereas a dentist may be more willing to undergo complex reconstruction and prolonged hand therapy to achieve optimal five-digit function. The preliminary evaluation is often limited because of significant pain and contamination. Nevertheless, it is imperative to assess all tissue systems, beginning with the vascular system, because the presence of compartment syndrome or hand ischemia requires emergent intervention.7 Early recognition and treatment of compartment syndrome is essential to prevent irreversible muscle and nerve damage. Patients may not be sufficiently lucid to express the cardinal signs of extremity pain exaggerated by passive stretching, because the extremity may already be too painful and injured to elicit these signs. Diagnosis is best confirmed by measurements of compartment pressures, with a pressure of more than 30 mm Hg commonly considered an indication for fasciotomy.8 If a commercial monitor is unavailable, a modified needle manometer technique can be performed with a straight 18-gauge needle, arterial line transducer, and central venous pressure monitor9 (Fig. 64.5). The injured hand should also be assessed for active bleeding and potential critical ischemia. Active bleeding is likely related to laceration of a major vessel. It is usually controlled with direct pressure and compressive dressing and, if necessary, short-term tourniquet application. Bleeding areas should not be blindly clamped, because this could damage neighboring neurovascular structures. Perfusion to the injured extremity is difficult to assess clinically because of extensive structural damage. A modified Allen test using a handheld Doppler probe is often necessary to assess patency of the major vessels, because patients with mutilating hand injuries may not be able to make a fist. Presence of vascular insufficiency will prompt immediate exploration and repair. When examining the skin, the degree of soft tissue loss, laceration, and contamination are noted to determine the amount of débridement and soft tissue coverage needed. Amputated parts should not be discarded, because they can serve as tissue donors for repair of other parts.10 Skin from an unsalvageable digit can be harvested with a neurovascular pedicle to provide sensate coverage to the adjacent defect. Bones can be used as grafts to add length to amputated digits. Tendon remnants can be used as grafts to bridge segmental defects or to reconstruct pulleys or ligaments. Fig. 64.5 (a) This 3-year-old boy presented with severe pain and a swollen hand 4 hours after an automobile ran over his hand. (b) A posteroanterior view of the hand revealed significant soft tissue swelling and fractures through the finger metacarpal bases. (c) A Stryker monitor was inserted into the first dorsal compartment and connected to a continuous central venous pressure monitor. (d) Intracompartmental pressure measurements were elevated up to 97 mm Hg. Evaluation of the skeletal system generally requires plain radiographs to confirm a clinical suspicion of skeletal injuries, to see any foreign bodies, and to note any previous healed fractures. Multiple views that include a joint above and below the level of injury should be obtained.1 Identification of unstable fractures and joint dislocations require immediate fixation and reduction. Delay in diagnosis can result in nonunion and joint instability. Underlying muscle–tendon unit injury can be appreciated by noting any deviation in the resting posture of the hand, which is maintained by normal flexor—extensor tendon balance.1 Lacerations of both digital flexor tendons results in the finger lying in extension while other fingers are in their normal flexion cascade. Laceration of the extensor tendons will result in wrist drop and lack of full extension of the involved finger. Nerve injury should be evaluated by testing motor and sensory function of the median, radial, and ulnar nerves. A useful method to rapidly assess motor function of all three nerves is by asking the patient to extend the wrist, abduct the middle and little finger, and make a ring sign with thumb and index finger touching each other11,12 (Fig. 64.6). Inability to extend the wrist indicates radial nerve injury, poor abduction of fingers suggests ulnar nerve weakness, and difficulty in opposing the thumb and index fingers reflects median nerve impairment. The sensory system is examined done by checking light touch in the sensory distribution of the three nerves. In the setting of open hand injuries, early surgical exploration is required to evaluate the continuity of the nerves. Blunt injury is associated with entrapment of the nerve from swelling and would benefit from surgical decompression, especially in the presence of evolving nerve deficits or very dense initial sensory deficits. Carpal tunnel syndrome is a common condition after a distal radial fracture; the surgeon should be cognizant of this fact and perform urgent release and fracture fixation when indicated.13 Fig. 64.6 Testing motor function of the hand. Assess motor function of all three nerves by asking the patient to make an “OK” sign. In general, the order of repair should be based on level of urgency, which is usually7: 1. Débridement 2. Skeletal fixation 3. Revascularization 4. Soft tissue coverage 5. Delayed nerve and tendon repair Adequate débridement is the cornerstone before any repair. Inadequate débridement results in infection, further tissue loss, and potential systemic complications. The next step is to stabilize fractures, because skeletal fixation provides the foundation for reconstruction. Restoration of bone alignment and length provides a solid base for anastomosing and grafting injured vessels and nerves. The bone is also the deepest structure and will be difficult to access if other superficial structures are repaired first. Joint stabilization helps provide smooth articulation and promote early rehabilitation, thereby minimizing joint stiffness. In the event of prolonged upper extremity ischemia in the proximal forearm or upper arm, revascularization should be done before operative débridement and bony fixation to decrease ischemia time and the attendant potential risks of myoglobinemia and muscle death with fibrosis. This is achieved using a temporary vascular conduit, and definitive revascularization is performed after skeletal reconstruction.14 Adequate, durable soft tissue coverage is as important as the reconstruction of the skeletal framework of the hand. Soft tissue replacement is performed as early as possible, because this minimizes the inflammatory reaction, scar formation, and wound contraction. Primary closure or delayed primary closure is preferred when feasible. The choice for soft tissue coverage is guided by the reconstructive elevator and is adjusted to fit the individual case. The decision is not always the simplest soft tissue reconstruction, but rather the technique that will ultimately achieve optimum form and function.15 Nerve and tendon repair should be delayed until stable soft tissue coverage is available. This minimizes the risk of tendon or nerve graft loss related to wound infection. The goals of reconstruction should be pliable soft tissue coverage, stable fracture fixation, supple joints and tendons, and good muscle function and distal digital sensibility.7 The surgeon should formulate a treatment plan that achieves both short- and long-term objectives. There should be realistic goals for anatomical and functional outcome. The basic plan, need for multiple surgeries, rehabilitation, and possible complications should be explained to the patient. Foreign material and necrotic tissue stimulate release of proteases, collagenases, and elastases that impede wound healing.16 In addition, bacteria produce wound-inhibiting enzymes and consume surrounding oxygen and nutrients. This environment inhibits macrophages’ ability to direct the formation of granulation tissue and neovascularization. Inadequate débridement will consequently result in wound infection and delayed wound healing. Adequate débridement begins with extensive irrigation and is followed by excision of the wound. The wound is initially cleaned using a surgical scrub brush and sterile soap followed by pulse lavage irrigation with sterile saline.17 Unless prolonged ischemia has already occurred, excisional wound débridement is best performed under tourniquet control with loupe magnification. Major neurovascular structures should be identified and tagged first. Wound excision is then performed layer by layer from the skin to the deeper tissues. Dead skin and fascia should be excised back to bleeding edges. Muscle viability should be assessed by color, contractility, and bleeding and excised if nonviable. Damaged ends of tendon should be débrided. Clinical judgment will then dictate immediate or delayed tendon repair or even reconstruction through grafts or tendon transfers. The ends of major nerves should be tagged for primary repair or delayed nerve grafting. Avascular bone fragments devoid of soft tissue attachment should be removed and bone ends débrided back to bleeding bone. The tourniquet should be released for reassessment of tissue viability, and further débridement is performed as needed. Although it may be necessary to perform serial débridement of contaminated wounds, progressive edema and granulation tissue will accumulate; therefore there should not be an undue delay in wound coverage. Early aggressive débridement is strongly advocated over traditional serial débridement whenever feasible.18 Wound vacuum-assisted closure (VAC) can provide temporary wound coverage while the wound is undergoing serial débridement or until a stable wound bed is achieved.19 It decreases buildup of edema and exudates to promote formation of granulation tissue. The surgeon should be mindful that a wound VAC does not result in optimal functional coverage and must have a definitive plan for soft tissue reconstruction. Complex fractures often occur with mutilating hand injuries and can result in malunion and nonunion if appropriate methods of bony fixation are not used. The optimal time for reduction and fixation is at the initial operation or within the first week to permit early mobility.7 K-wires provide rapid stabilization of digital fractures with the least amount of additional soft tissue damage. However, they do not provide rigid fixation for early mobility, and collapse may occur at the fracture site, resulting in misalignment.20 Miniplates or interosseous wires offer stable fixation but are more technically challenging and require additional soft tissue dissection. In the setting of extensive contamination or bone loss, external fixation may be the method of choice for temporary skeletal stabilization. The fixators should be positioned so that they will not interfere with future soft tissue reconstruction. Metacarpal and phalangeal fracture malunions can be repaired by corrective osteotomy at the prior fracture site and may accompany simultaneous tenolysis and capsulotomy.21 Nonunions can be treated with cancellous bone graft from the radius or iliac crest and maintained in place with a compression plate. Among the most difficult challenges in the management of mutilating hand injuries is the decision between amputation and limb salvage. Amputation is undoubtedly an unpleasant and devastating event; on the other hand, salvage of a stiff, painful, and insensate limb can be more detrimental. McCormack22 found that irreparable damage to three or more of the five tissues in the hand may be a strong indication for early digit amputation. The best time to perform primary amputation is at the initial operation. Delayed amputation is associated with adverse psychological effects and an inferior functional result.23 Understanding the biomechanics of the hand is crucial in determining what anatomic components are needed for hand function. The minimal elements for the hand include the thumb and two digits for three-point stability24 (Fig. 64.7). This allows for prehension, which requires opposition between the thumb and fingers to coordinate pinch. The American Medical Association Guidelines of Permanent Impairment25 estimates that loss of the thumb is equivalent to a 40% loss of hand function, which makes it the most important digit to preserve and reconstruct. For the most part, loss of the distal phalanx and interphalangeal joint produce minimal functional deficit of the thumb, whereas injuries at or proximal to the MCP joint may require toe transfer or distraction lengthening to maintain oppositional function. The index finger has a major role in precision pinch and directional grip but has little function if amputation exists proximal to the PIP level and when there is minimal MCP motion remaining. Under these circumstances, ray amputation can often improve function by opening the first web space, and its function is then taken over by the middle finger.7 The middle and ring fingers provide grip and grasp functions. After amputation of the middle finger, grip is weakened because of loss of the three-point chuck pinch. Small objects can also fall from grasp through the space left by the missing digit. Transposition of the index finger to the amputated middle finger can be performed to widen the first web space and close the gap and to achieve better prehension and aesthetic appearance26 (Fig. 64.8). Despite the least strength in flexion, the little finger defines hand width for grip functions and has been reported to have the greatest functional value after the thumb. In general, single-digit amputation other than the thumb does not result in substantial loss of hand function.
64
Soft Tissue Coverage and Mutilating Extremity Injuries

Avoiding Unfavorable Results and Complications in the Treatment Of Mutilating Injuries
Missed Diagnosis and Delayed Treatment
Missing Life-Threatening Injuries
Underestimating the Severity of Injury
Incomplete Patient History
Missing Limb-Threatening Injuries
Discarding Spare Parts
Missing Fractures and Dislocations
Missing Tendon Injuries
Missing Nerve Injuries

Prioritization of Repair
Managing Unfavorable Results and Complications in the Treatment of Mutilating Injuries
Complications of Inadequate Débridement
Wound Infection and Delayed Wound Healing
Delayed Wound Closure
Complications of Skeletal and Joint Repairs
Malunion and Nonunion
Failure to Proceed with Primary Amputation
Plastic Surgery Key
Fastest Plastic Surgery & Dermatology Insight Engine